Role of concomitant percutaneous pie crusting and local corticosteroid injection in lateral epicondylitis: a prospective, case control study
Article information

Abstract
Background
Lateral epicondylitis is an increasingly debilitating condition in working population. Evidence for conservative treatment modalities has been inconclusive. Percutaneous pie crusting of the common extensor origin at the lateral epicondyle at the time of local corticosteroid injection (CSI) has been proposed sparsely. The objective of this study was to analyze if concomitant CSI and pie-crusting of the common extensor origin provides better outcome than CSI alone in lateral epicondylitis.
Methods
This case-control study on 236 patients was conducted at a single center between January 1, 2020, and May 31, 2022. Patients were divided into two groups (n=118 each) based on their preference. Group A underwent CSI alone and group B underwent pie crusting along with CSI. The clinical and functional outcomes of all patients were evaluated at 2, 4, 6, and 12-week post-procedure using the visual analog scale (VAS) and Nirschl score. The mean time for return to daily activities was also compared.
Results
Both groups showed significant improvement in post-procedure outcome at successive follow-ups on intragroup longitudinal analysis (VAS: F=558.384 vs. F=1,529.618, Nirschl: F=791.468 vs. F=1,284.951). On intergroup analysis, VAS of group B was superior to that of group A; however, it was statistically significant (P<0.05) only from the 6-week follow-up onwards. Nirschl score of group B was significantly better throughout the period of follow-up (P<0.05). Group B returned to daily activities faster than Group A (6.2±0.44 weeks vs. 7.18±0.76 weeks).
Conclusions
Concomitant pie crusting with CSI is recommended for lateral epicondylitis as it provides significantly better results than CSI alone.
Level of evidence
III.
INTRODUCTION
Lateral epicondylitis is a medical condition that causes pain on the lateral side of the elbow and is aggravated by wrist extension [1]. The incidence varies from 1% to 3% [2]. While the exact pathophysiology behind the condition is unclear, and despite the presence of inflammatory cells locally, there is a strong argument that lateral epicondylitis is a degenerative process caused by muscle overuse, with subsequent tendinosis, micro-trauma and fraying of the extensor carpi radialis brevis tendon [3,4]. This disorder was first described by Runge in 1873 [5,6]. In 75% of cases, the dominant side is affected, suggesting that work-related forceful and repetitive wrist extension may have a role in the pathogenesis of the "repetitive strain injury” [7]. The most common etiology is microscopic tears with formation of reparative tissue on the lateral epicondyle [6].
The management of lateral epicondylitis has evolved over the last two decades. According to the current literature, lateral epicondylitis is treated successfully by nonoperative measures approximately 90 % of the cases [8,9]. The current available treatment methods include acupuncture, ultrasonography, steroid injections, counterforce bracing, stretching exercises and cross-frictional massaging. The more successful nonoperative treatment consists of avoidance of overuse, counterforce bracing to relieve the insertion site of the extensor tendons, steroid injection into the affected area and stretching exercises [10]. Acupuncture, cross-frictional massage, and ultrasonography are symptomatic modalities that provide short term pain relief requiring multiple sittings and are ineffective as standalone options. Despite their good reported outcomes, counterforce bracing and stretching exercises are time-consuming treatment options and patient compliance, proves to be a stumbling block [8-10].
There are a relatively large number of treatment options available for the treatment of lateral epicondylitis. However, there is the sparse evidence available about the disease etiology and a lack of agreement about the definitive treatment protocols in its management. There is also an increased demand from patients, especially in the working-class population, for a treatment modality that provides faster relief and facilitates earlier return to normal daily activities. One of the proposed methods of management is local corticosteroid injection (CSI) at the most tender point over the affected humeral lateral epicondyle; however, it has been shown to have varied results. Percutaneous pie-crusting has been proposed as a viable treatment option for lateral epicondylitis owing to its ability to release taut myofascial bands, improve microcirculation and relieve myofascial trigger points. The combination of these effects with pie-crusting with the anti-inflammatory action of the steroid injection could prove to be a good conjunct for better and more consistent results. This has not been studied extensively. We hypothesize that in cases with persistent signs and symptoms of lateral epicondylitis, administering CSI along with pie crusting of the common extensor origin may improve the clinical outcome and provides a relatively pain free return to daily life activities compared with CSI alone.
METHODS
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008 (5). The study was conducted in a private setup and hence institutional review board approval was not required. Written informed consent was obtained from all individual participants included in the study.
Study Design
This prospective, case-control study was conducted at a single center between January 1, 2020, and May 31, 2022. A total of 348 consecutive patients who were clinically diagnosed with lateral epicondylitis were included in the study. The advantages and potential drawbacks of all treatment modalities, including counterforce bracing and stretching, CSI, and CSI with pie-crusting, were explained to all patients. Of the 348 patients, 89 patients opted for counterforce bracing while 259 patients opted for either isolated CSI or concomitant CSI and pie crusting. From the total group, 20 patients were excluded based on the predetermined exclusion criteria and three patients were excluded following matching of the groups. Patients were divided into two groups based on their preferences. Group A (n=118) underwent CSI alone and group B (n=118) underwent pie crusting along with CSI. The patients were included in the study based on fixed inclusion and exclusion criteria.
Patient Population
The inclusion criteria were as follows: the age of 18 years clinically diagnosed as a case of lateral epicondylitis using positive Cozen’s, Maudsley’s and Chair lift test and confirmed on ultrasound imaging, and duration of symptoms no more than 6 months [4,11-13]. The exclusion criteria was as follows: patients with localized skin conditions, patients with history of previous elbow or periarticular fracture, dislocation or surgery as confirmed by ultrasound, use of acetylsalicylic acid and/or non-steroidal anti-inflammatory drug (NSAID) within 7 days before the procedure, previous history of any form of local injection or invasive therapy at the same site since onset of symptoms, recurrent or recalcitrant cases, active local or systemic infection, central or peripheral nervous system disease, patients on blood thinners or suffering from blood dyscrasias, patient with further degenerative changes of the elbow contributing to pain, such as cartilage thinning, loose body, or evidence of tendinosis other than medial or lateral, including triceps or ulnar collateral ligament on ultrasound, patients with other inflammatory arthritis and other elbow pathologies like rheumatoid arthritis, osteoarthritis, hyperuricemia, or radial tunnel syndrome and, patients with calcification on lateral epicondyle on ultrasound.
Baseline demographics and clinical scores were matched for both the groups to eliminate bias (Table 1). Group A was given CSI (3 mL of 2% plain lignocaine and 2 mL [80 mg] of Methylprednisolone) alone over the most tender point over the lateral epicondyle. Group B underwent concomitant pie crusting of the lateral epicondylar aponeurosis and CSI over the most tender point over the lateral epicondyle. The functional outcome assessment before the procedure was performed using visual analog scale (VAS) and Nirschl scores (Table 2).
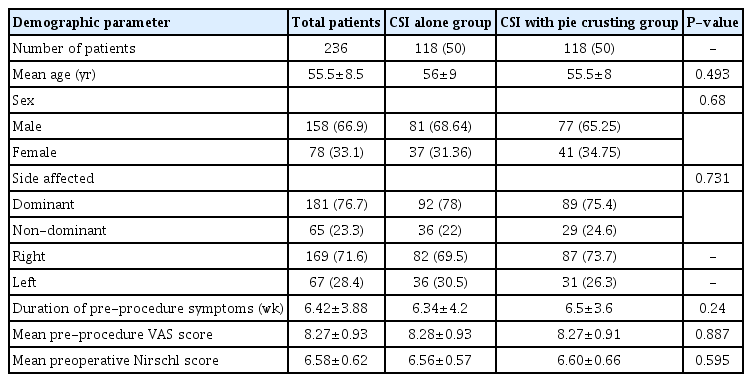
Baseline demographic and clinical data of patients in the local CSI alone and CSI with pie crusting groups
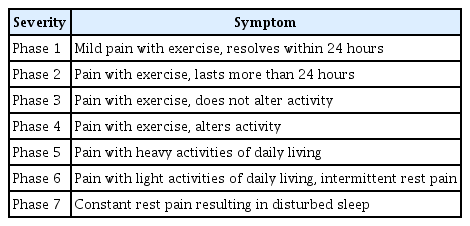
Nirschl score
Procedure Technique
A test dose of 2% plain Lignocaine from a multidose vial was injected intradermally to check for any hypersensitivity reaction before the procedure. None of the patients tested positive for lignocaine hypersensitivity. The procedure was conducted by the primary author on an outpatient basis. With the patient in supine position over the examination bed and the affected forearm resting over a pillow by the side, the elbow was flexed to 90º. The region over the lateral epicondyle of the affected elbow was cleaned with Betadine solution and Sterilium (propanol and macetronium ethylsulphate solution) and all aseptic precautions were maintained. The most tender point over the lateral epicondyle was palpated. The bevel of the 23-G needle was inserted perpendicular to the skin anterior to the lateral epicondyle. Simultaneous injection of 3 mL of 2% plain lignocaine and 2 mL (80 mg) of the methylprednisolone mixture with percutaneous pie crusting of the common extensor origin was carried out for the appropriate patients (Fig. 1); otherwise, only CSI was given (Fig. 1C). By moving the tip of the needle circumferentially, the lateral epicondyle pie crusting (repeatedly creating fenestrations in the tendinotic tissue) of the common extensor origin aponeurosis was performed with a grating sensation indicating the correct anatomical location. The adjacent bony surface of the apex and face of the lateral epicondyle were abraded. After the procedure a small waterproof dressing pad was applied (Supplementary Video 1).
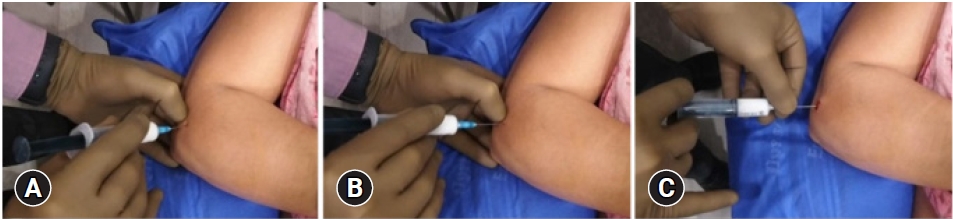
(A) Introduction of the 23-G needle at the most tender point of the lateral epicondyle under aseptic precautions. (B) Circumferential pie crusting over the common extensor origin aponeurosis. (C) Combination of 2 mL (80 mg) methylprednisolone and 3 mL of 2% plain lignocaine injected into the most tender point over the lateral epicondyle.
All the patients were advised ice fomentation in case of pain and wear a counterforce brace as a prophylactic measure to reduce pain and inflammation and encourage faster rehabilitation for 6 weeks. They were instructed not to lift any weights until advised. After the procedure, the patients were put on a 5-day course of oral antibiotics. No analgesics were given to avoid masking of pain. Patients were followed up at 2 weeks, 4 weeks, 6 weeks, and 12 weeks. No patients were lost to follow-up.
Study Outcome Assessment
Function was measured by Nirschl score and pain intensity was measured by VAS score; mean duration to return to daily activities (time taken to perform all of the following activities painlessly: opening a door, lifting a glass, turning a key, getting up with support, taking a bath, traveling in public transport, cooking, and maintaining hygiene) post-procedure, and complications such as recurrence and infection were evaluated. All outcomes were compared between the pie-crusting and no pie-crusting group at 2, 4, 6, and 12 weeks post-procedure to determine the efficacy of concomitant pie crusting and CSI as compared to isolated CSI. Patients lost to follow-up during the 12 weeks of follow-up were excluded from data analysis. None of the patients reported any complications.
VAS for pain and Nirschl elbow score were determined by a blinded clinician [5]. Nirschl score describes the phases of pain and its correlation with activity level in patients with lateral epicondylitis, with phase 0 being no pain or soreness and phase 7 being moderate or greater pain before, during and after any activity forcing the patient to stop the activity along with rest pain and night pain disturbing sleep [5].
Statistical Analysis
Statistical analyses were performed using the SPSS ver. 24 statistical software (IBM Corp.). Baseline demographic and clinical variables such as age, gender, dominant side affected, duration of symptoms, pre-procedure VAS, and Nirschl score were compared and matched between the two groups. Longitudinal intragroup analysis was done using repeated measure analysis of variance test, and intergroup assessment at each follow-up was done using Mann-Whitney U-test. A P-value <0.05 was considered to be significant. The power of the study for a sample size of 236 was calculated to be 100% retrospectively, keeping alpha as 0.05 and adjusted R squared as 0.669 for Nirschl score as a dependent variable and adjusted R squared as 0.642 for VAS score as a dependent variable.
RESULTS
A total of 236 patients were included in the study, including 158 men (66.9%) and 78 women (33.1%). The mean patient age was 55.5±8.5 years (range, 41–64 years). The demographic data of the sample size are shown in Table 1. The average time from the onset of symptoms was 6.42±3.88 weeks. Baseline variables such as mean age (P=0.493), gender distribution (P=0.680), dominant side affected (P=0.731), mean duration of symptoms (P=0.240), mean pre-procedure VAS (P=0.887) and Nirschl score (P=0.595) were similar in the two groups.
Both groups showed similar post-procedure trends on intragroup longitudinal analysis with significant improvement at every follow-up compared with the previous follow-up and pre-procedure scores, irrespective of whether pie-crusting was done or not. In intergroup analysis, the VAS score of pie crusting group was superior to its counterpart; however, it was statistically significant (P<0.05) only from the 6-week follow-up onwards. In terms of Nirschl score, the pie crusting group was significantly better than the no pie crusting group throughout the follow-up (P<0.05) (Table 3). The mean time to return to daily activities was faster in the pie crusting with CSI group compared with the CSI alone group (6.2±0.44 weeks vs. 7.18±0.76 weeks, P=0.024).

Clinical outcomes in the local CSI alone and CSI with pie crusting groups
DISCUSSION
Our study demonstrated that concomitant CSI and pie crusting is beneficial in terms of superior outcome compared with local CSI alone in cases of lateral epicondylitis. Lateral epicondylitis is a relatively common and debilitating upper extremity problem [14]. The etiology is attributed to various factors like bursitis, synovitis, ligament inflammation, and periostitis; the most common accepted etiology is microscopic tears with formation of reparative tissue on the lateral epicondyle [15].
The principle underlying any successful procedure is the accurate identification of the pathological process involved and its correction with a minimum disruption of normal tissues. The treatment of lateral epicondylitis has been laden with controversy. Several interventions and treatment have been described and explored for faster recovery and healing. Topical NSAIDs, local CSI and extracorporeal shock wave therapy are likely to be beneficial for short-term pain relief and improvement in function. For chronic and recalcitrant cases of lateral epicondylitis, various surgical techniques including fasciotomy, Z-lengthening of the tendon, osteotomy of the lateral epicondyle, and excision of the damaged portion of extensor carpi radialis brevis as well open and percutaneous tenotomy have been described in the literature.
Sims et al. [16] observed that 92% of patients had a good functional outcome after CSI at 4 weeks compared with 50% of patients treated conservatively with oral NSAIDs and physiotherapy. These results were also congruent with our study regarding improvement in the functional outcomes at 4 weeks after concomitant CSI and a supplementary pie crusting further improving the outcome in cases of lateral epicondylitis. Sims et al. [16] noted that at the 6-week follow-up, the injection group fared significantly better in all outcome measures (92% success vs. 47% for physiotherapy and 32% for wait-and-see). We noted that patients who underwent concomitant CSI and pie crusting showed even better results at the 6-week follow-up compared with CSI alone.
We opted for a combination of 2 mL (80 mg) methylprednisolone and 3 mL of 2% plain lignocaine injected into the most tender point over the lateral epicondyle followed by concomitant pie crusting to provide pain relief to accelerate range of motion recovery [17]. The general anti-inflammatory action of corticosteroids, along with their ability to obtund proliferation of the aponeurosis and fibrosis, makes it an efficient tool to directly reduce the incidence, as well as the progression of post-procedure elbow pain and stiffness [18,19]. We hypothesize that concomitant pie crusting of the extensor tendon sheath gives improved results in the backdrop of anti-inflammatory action of corticosteroids by releasing the taut myofascial bands secondary to the inflammation, increasing microcirculation, thereby improving the healing process, and consequently causing symptomatic pain relief. The timing of pie crusting and an CSI for lateral epicondylitis is a matter of debate [20].
We hypothesize a direct correlation between the pain subsidence following a combination of pie crusting and the CSI and better compliance in regaining activities of daily life compared with CSI alone. No hypersensitivity reactions to the corticosteroid injection, acute or delayed, were noted in any patient. No signs of infection such as redness over skin, local rise in temperature, or painful range of motion was found in any patient at any follow up, indicating the absence of infection.
This study has several limitations, such as the limited geographical area covered for sample collection, short follow-up period, potential observer error (as all patients were evaluated by a single blinded clinician), and reproducibility of the procedure. However, the study holds value in terms of fortifying the safety and efficacy of the combination and determining the site of the injection. This article introduces a new method of pie crusting technique, which is safe and potent. As all baseline data was matched and the evaluating clinician was blinded, most of the biases were accounted for. The 100% power of the study further adds to the authenticity and value of the findings.
In conclusion, compared with CSI alone, a single injection of 2 mL (80 mg) methylprednisolone and 3 mL of 2% plain lignocaine combined with percutaneous pie crusting of the aponeurotic bands gives better results in cases of lateral epicondylitis and enables early return to daily activities, irrespective of the time since onset of symptoms.
Notes
Author contributions
Conceptualization: AMR.Data curation: ARSM, VK. Formal Analysis: ARSM, KR. Funding acquisition: KR. Investigation: ARSM, VK. Methodology: AMR. Project administration: KR. Resources: KR. Software: ARSM, KR. Supervision: AMR. Validation: ARSM, VK. Visualization: KR. Writing – original draft: ARSM, VK. Writing – review & editing: AMR, ARSM, KR, KR.
Conflict of interest
None.
Funding
None.
Data availability
Contact the corresponding author for data availability.
Acknowledgments
None.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.5397/cise.2022.01375.
Supplementary Video 1.
Video demonstration of the technique of simultaneous pie crusting and local corticosteroid injection.
cise-2022-01375.v1.mp4