Reliability of the scapular dyskinesis test yes-no classification in asymptomatic individuals between students and expert physical therapists
Article information

Abstract
Background
Scapular dyskinesis is considered a risk factor for the shoulder pain that may warrant screening for prevention. Clinicians of all experience screen scapular dyskinesis using the scapular dyskinesis test yes-no classification (Y-N), yet its reliability in asymptomatic individuals is unknown. We aimed to establish Y-N’s intra- and inter-reliability between students and expert physical therapists.
Methods
We utilized a cross-sectional design using consecutive asymptomatic subjects. Six students and two experts rated 100 subjects using the Y-N. Cohen’s kappa (κ) and Krippendorff’s alpha (K-α) were calculated to determine intra- and inter-rater reliability.
Results
Intra- and inter-rater values for experts were κ=0.92 (95% confidence interval [CI], 0.91–0.93) and 0.85 (95% CI, 0.84–0.87) respectively; students were κ=0.77 (95% CI, 0.75–0.78) and K-α=0.63 (95% CI, 0.58–0.67).
Conclusions
The Y-N is reliable in detecting scapular dyskinesis in asymptomatic individuals regardless of experience.
INTRODUCTION
Optimal shoulder function requires proper positioning and movement of the scapula on the thorax [1]. Abnormal scapular position or movement patterns during functional activities are defined as scapular dyskinesis [2,3]. Although it is typically associated with shoulder pain [4-6], dyskinesis also can be present in asymptomatic individuals [7-9]. More recent evidence suggests that scapular dyskinesis is a risk factor for shoulder pain [10] that may warrant screening as a preventative measure.
Physical therapists screen for scapular dyskinesis by visually comparing scapular movement asymmetries in overhead reach using the Scapular Dyskinesis Test [3]. The patient performs repeated shoulder elevation and lowering with weights on both hands while the therapist observes scapular motion. The therapist identifies and labels scapular dyskinesis as type 1 when there is an excessive prominence of the inferior angle, as type 2 when there is excess prominence of the medial border or dysrhythmia, or as type 3 with excessive or premature movement of the scapula observed on a single plane of motion. The large numbers of possible abnormal movement patterns and combinations can make it difficult for therapists to agree on a final label. A variant of the test known as the Yes-No classification (Y-N) simply identifies the presence or absence of asymmetry between the shoulders and is more inclusive without need for the therapist to observe multiple separate planes, increasing the reliability [11]. The improved accuracy of the Y-N may be due to its simplicity and dichotomous decision [12]. Novice clinicians, such as physical therapy students, can quickly learn the Y-N as part of their training (e.g., clinical rotations). However, the Y-N involves subjectivity in that it relies heavily on clinician experience and is an observational method [13]. As novices, physical therapy students lack the experience needed for reliable and accurate measurement based on academic and clinical standards, especially in shoulder assessment tools [14,15]. Many studies have compared the reliability between novices and experienced clinicians using other assessment tools (primarily in balance) in physical therapy [16,17]. These studies also found evidence of rater discrepancy due to lack of experience. The Y-N has shown reliability among experienced clinicians [11,18,19]. However, its reliability across varied clinical experiences in the asymptomatic population is unknown.
Therefore, we aimed to determine the intra- and inter-rater reliability of the Y-N in detecting scapular dyskinesis in asymptomatic individuals between students and expert physical therapists. We hypothesized that the Y-N is a reliable tool in detecting scapular dyskinesis among asymptomatic individuals when used by experts but not by students due to lack of experience.
METHODS
Approval was obtained from the Institutional Review Board of Augusta University, and all subjects read and signed a consent form before participating in our study. Especially, the authors obtained consent from the participant whose body was exposed in the figure.
Study Design
A cross-sectional intra- and inter-rater reliability design was utilized.
Subjects
Participants were conveniently sampled from students on the Health Sciences campus of Augusta University. Asymptomatic adults 18–35 years old were recruited using word of mouth and referrals. Table 1 summarizes the exclusion criteria. A screening tool for eligibility included existing medical problems, medications, and pain ratings. The first consecutive 100 healthy asymptomatic subjects that met the criteria were included in the study and underwent evaluation via the Y-N (see Procedures and Instrumentation). Table 2 summarizes the demographic characteristics of the subjects.
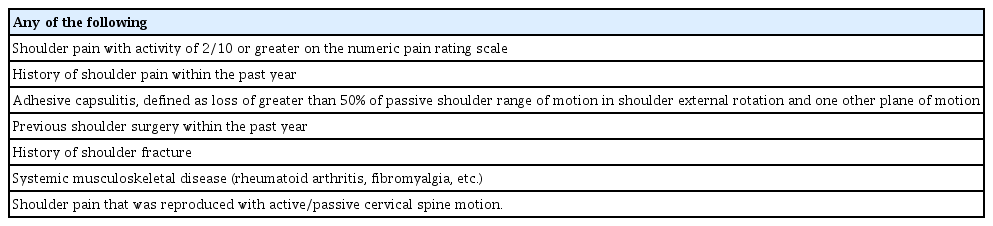
Exclusion criteria

Demographic characteristics of the subjects
Raters
There were eight raters: two experts and six students. The expert raters were licensed and certified orthopedic physical therapy specialists, one with 25 years of clinical experience, considered the expert gold standard, and the other with 21 years of clinical experience. The student raters were second-year PT students. All raters were blinded to other’s data during the study period. Table 3 summarizes the demographic characteristics of the raters.

Demographic characteristics of reliability study raters
Procedures and Instrumentation
Scapular dyskinesis test yes-no classification
The Y-N was performed on the 100 subjects and video recorded for later evaluation of presence or absence of scapular dyskinesis (Fig. 1). Male participants were asked to remove their shirts, while women wore sports bras to expose both scapulae. Using a metronome at a rate of 60 beats per minute, participants performed five consecutive non-stop repetitions of bilateral, active, and weighted 120º shoulder flexion using dumbbells based on body weight: 1.4kg (3lb) for those weighing <68.1 kg (150 lb) and 2.3 kg (5 lb) for those >68.1 kg (150 lb) according to the scapular dyskinesis test protocol by McClure at al. [18].
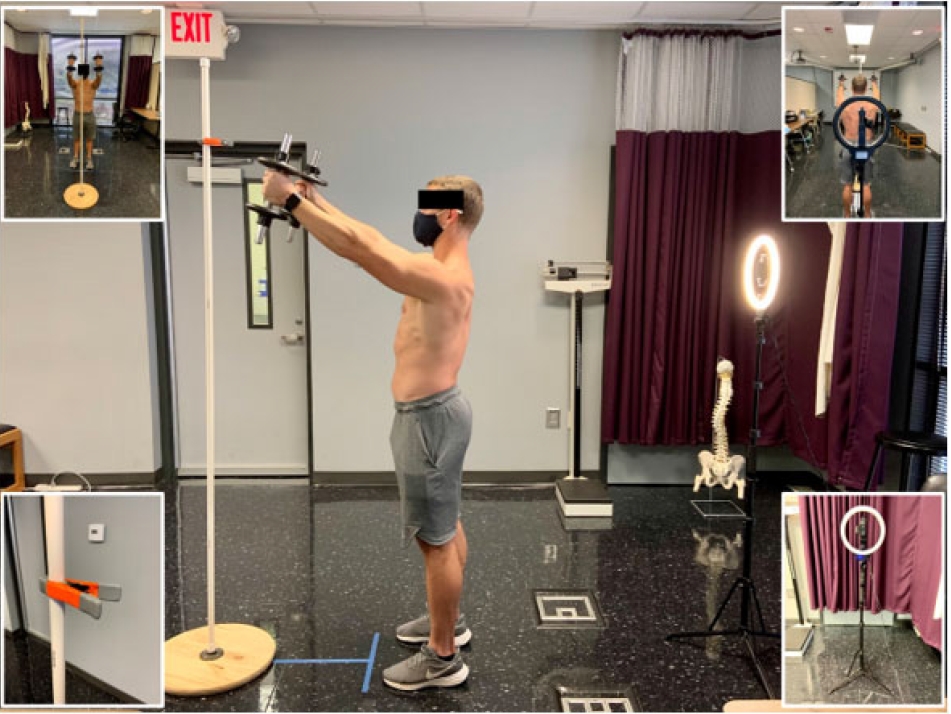
Scapular dyskinesis test yes-no classification and video recording set-up.
An eight-foot PVC pipe on a wooden base was placed in front of the subjects (two feet from their toes) to standardize shoulder flexion and assure accuracy among the five repetitions. A spring clamp with handles wrapped with bright neon orange tape was clamped to the pole for easy visibility. Subjects’ shoulders were passively elevated to align with a goniometer (fixed at 120º) and were held in that position. The clamp was moved roughly at the level of the subjects’ middle fingers or a level they would remember to raise their arms during the test. To establish reliability between repetitions, after determining the clamp's ideal height on the pole, subjects were asked to put their arms to their sides, raise them again to the clamp level, and hold. The fixed goniometer was placed at the shoulders one at a time to verify alignment. This process was repeated until elevation of both arms aligned with the goniometer.
To record the movement, a high-definition digital camera on a tripod equipped with lighting was set up one meter behind the participant at the level of the seventh thoracic spinous process (between the inferior angles of the scapulae). Each video was saved in an MP4 format and labeled with an unidentified subject number assigned during the consent process. All videos were stored in a secure Box folder (server) provided by the Institutional Review Board. After watching the videos independently, raters used the Y-N to label the presence or absence of scapular dyskinesis for each subject they evaluated.
Definitions of operational terms
Yes: Scapular dyskinesis is present (asymmetrical shoulders). Either or both of the following motion abnormalities may be present on either shoulder: (1) dysrhythmia: the scapula demonstrates premature or excessive elevation or protraction, non-smooth or stuttering motion during arm elevation or lowering, or rapid downward rotation during arm lowering or (2) winging: the medial border or inferior angle of the scapula is posteriorly displaced from the posterior thorax.
No: Scapular dyskinesis is not present (symmetrical shoulders). Both scapulae are stable with minimal motion during the initial 30º to 60º of shoulder elevation. Smooth and continuous scapular rotation upward during elevation and downward during humeral lowering. No evidence of winging.
Student training
Students underwent a two-part standardized training provided by the expert gold standard (Fig. 2). The first part was a didactic format to educate the students on use of the Y-N. The second part was a practical application format where all student raters independently rated sample videos of subjects performing the Y-N to achieve a baseline minimum of substantial agreement (Krippendorff’s alpha or K-α=0.61–0.80) [20] before the study proper.

Student rater training. SYM: symmetrical, ASYM: asymmetrical, K-α: Krippendorff’s alpha.
Rating process
After reaching the required baseline level of agreement (substantial) among the six student raters, the 100 study videos were released to all raters at a rate of 10 per week over the next 10 weeks for independent rating. The ratings in this part were used to calculate inter-rater reliability. Access to the videos was closed and the ratings were due at the end of the week. At the end of the 10th week, videos from the first week were re-released for the second round of ratings. Ratings in this part were used to calculate intra-rater reliability.
Sample size estimation
A priori power analysis using Real Statistics Resource Pack software, release 7.2, was used to establish reliability. Based on the previously determined inter-reliability Cohen’s kappa (κ) value of 0.64 [21] with a significance level of 0.05 and power of 90%, the minimum sample size required to test the null hypothesis κ=0.3 versus the alternative hypothesis κ=0.6 was 72.
Statistical Methods
To determine the intra-rater reliability in student and expert raters, κ [22] and its 95% confidence interval (CI) for each rater were calculated between the first and second ratings of the videos from the first week (10 weeks apart) and then averaged. To determine the inter-rater reliability between student raters only, κ-α [23] with its 95% CI was calculated. To determine the inter-rater reliability between expert raters only, the κ was calculated. Bootstrapping using the nonparametric (resampling) method, with a sample size of 1,000 that yielded 1,500 pairs, was performed to improve the accuracy of distribution of the alphas and Kappas [20,24]. Without bootstrapping, the CIs were wider (Table 4). The suggested interpretation of both K-α and κ is as follows: <0.0, poor agreement; 0.0–0.2, slight; 0.21–0.4, fair; 0.41–0.6, moderate; 0.61–0.8, substantial; and 0.81–1, near-perfect [22]. Statistical significance was set at α=0.05. Statistical tests were performed with IBM SPSS ver. 27 (IBM Corp., Armonk, NY, USA).
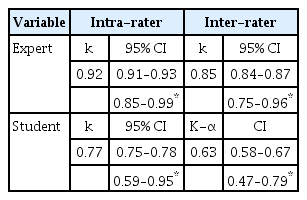
Summary of rater reliability
RESULTS
Experts and students were reliable in using Y-N to detect scapular dyskinesis in asymptomatic individuals. Table 4 summarizes the reliability results of experts and students. The intra-rater reliability of the experts was near perfect (κ=0.92), while that of students was substantial (κ=0.77). The inter-rater reliability of the experts also was nearly perfect (κ=0.85), and that of the students remained substantial (K-α=0.63). The prevalence rate of scapular dyskinesis in our sample of 100 subjects as identified by the experts was 59%.
DISCUSSION
The results showed that the Y-N was reliable when used by students or experts in subjects without shoulder pain. Although student reliability was substantial, there was a 20-point difference from experts with near-perfect reliability. This was consistent with similar studies that investigated student reliability compared to that of experts using other clinical tests [16,17,25]. This finding was not surprising as experience may be the most obvious explanation for such a discrepancy. All authors of these studies concluded that experience was the most significant factor that explained the difference.
Our study found that reliability among students was consistently substantial when the Y-N was applied to asymptomatic subjects. This was consistent with the findings of a similar study by Møller, with student κ scores in the range of 0.70–0.90 [12]. Although their research also used PT students as raters, their reliability scores were higher than those of our study. This could be because they used PT students in their final year instead of PT students in their second year. This difference emphasizes the importance of clinical experience.
Our study found that expert reliability was consistently near perfect when the Y-N was applied to asymptomatic subjects. In a previous study by Uhl et al. [11] utilized the Y-N for measuring reliability, the kappa score was only moderate between experts (κ=0.41). Interestingly, the definition of “expert” in the Uhl et al.'s study [11] was limited to “experienced clinicians.” In contrast, we defined experts as those board certified in orthopedic physical therapy and with at least two decades of clinical experience. This indicates that experience remains the most significant defining factor for higher reliability, even among experts. This was the same as the conclusion of Lluch et al. [26] in their comparison of inter-rater reliability among licensed physical therapists with different levels of experience.
Our study prevalence rate of scapular dyskinesis among asymptomatic individuals was 59%. It has been reported that about 60%–70% of individuals suffering shoulder pain have scapular dyskinesis [7-9]. However, many of those studies reported a similar proportion of patients with scapular dyskinesis even among healthy asymptomatic individuals reflective of our study’s prevalence result.
The Y-N is very subjective, and there is possibility of an expectation bias because of an expected outcome. This may have influenced the scapular dyskinesis labeling because raters “see what they want to see;” in this case, the presence of scapular dyskinesis.
Most of the experiments took place during the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic [27]. The rating period stretched over 10 weeks at the pandemic height, which may have introduced history and timing biases from subject recruitment to rater performance.
Use of convenience sampling and its associated sampling bias may contribute to the weak generalizability of the results. It is possible that the sample was not representative of the general population due to the nature of volunteer subject enrollment and its associated response bias.
In conclusion, the Y-N is reliable in detecting scapular dyskinesis regardless of experience level when used in an asymptomatic population for screening.
Notes
Financial support
None.
Conflict of interest
None.