Good functional results with open reduction and internal fixation for locked posterior shoulder fracture–dislocation: a case series
Article information

Abstract
Background
There is no standardized therapeutic strategy for locked posterior shoulder fracture–dislocation (PSFD), and no consensus exists on the analysis of preoperative factors. This retrospective study aimed to evaluate functional results and complications in a series of PSFD cases managed with open surgical treatment.
Methods
Patients diagnosed with locked PSFD who underwent open surgical treatment with reduction and osteosynthesis between April 2016 and March 2020 were included. All participants were treated with open reduction and internal fixation. Functional assessment used the modified University of California, Los Angeles (UCLA) mod scale, American Shoulder and Elbow Surgeons (ASES) questionnaire, subjective shoulder value (SSV), and visual analog scale (VAS). Complications were evaluated clinically and radiologically by X-ray and computed tomography.
Results
Twelve shoulders were included (11 patients; mean age, 40.6 years; range, 19–62 years). The mean follow-up duration was 23.3 months (range, 12–63 months). The UCLA mod, ASES, SSV, and VAS scores were 29.1±3.7, 81.6±13.5, 78±14.8, and 1.2±1.4 points, respectively. The overall complication rate was 16.6%, with one case of post-traumatic stiffness, 1 case of chronic pain, and no cases of avascular necrosis.
Conclusions
Open surgical treatment of locked PSFD can achieve good functional results. A correct understanding of these injuries and good preoperative planning helped us to achieve a low rate of complications.
INTRODUCTION
Locked posterior shoulder dislocation (LPSD) is a rare injury [1] associated with electric shocks, seizures, or high-impact injuries [2-4]. LPSD can be underdiagnosed because the clinical and imaging patterns may not be as clear as those of anterior shoulder dislocation [5], which unfortunately has a negative effect on prognosis. The most common associated injury is an impaction fracture of the anterior humeral articular surface, known as “reverse Hill-Sachs (RHS),” also called a simple posterior shoulder fracture–dislocation (PSFD). Cases involving a fracture of the anatomic/surgical neck or tuberosities are considered complex PSFD [2,4,6-8].
The most critical factors for therapeutic planning for a PSFD are the size of the RHS lesion, temporality, and type of associated fracture [9]. However, the analysis of these factors remains controversial [4]. Correct measurement of an RHS lesion is still under discussion [10,11]. This allows classification of joint involvement according to size (mild, <25%; moderate, 25%–50%; and severe, >50%) to guide the choice of treatment option. The time from injury has also been defined in various ways in the literature. According to the European Federation of National Associations of Orthopaedics and Traumatology [12], for an “acute” injury, the time from injury to surgery (TFIS) should be <3 weeks from the initial trauma; for a “neglected” injury, the time should be 3–6 weeks; and, for a “chronic” injury, the time should be >6 weeks [7,13]. Finally, management of associated fractures adds complexity and is still under discussion among surgeons [2,4,14]. For these reasons, multiple treatment options have been described for these patients (e.g., reverse fill, modified McLaughlin, auto/allograft, arthroplasty) [4,7,12,15,16]. To date, there is no standardized therapeutic strategy, and no consensus has been reached on the analysis of preoperative factors due to the lack of cohort studies with a high level of evidence.
The primary aim of this study was to evaluate the functional outcomes of a case series of patients treated for locked PSFD with open reduction and internal fixation (ORIF). The secondary aim of this study was to describe the incidence of complications and the re-intervention rate in these patients. The study hypothesis was that good functional results and a low rate of complications can be achieved with early and standardized open surgical treatment.
METHODS
Approval for this study was obtained from the Ethics Committee of Hospital del Trabajador. The procedures used in this study adhered to the tenets of the Declaration of Helsinki. All patients provided informed written consent for participation in the study and eventual publication.
Demographic Characteristics of the Patients
This was a retrospective study. Between April 2016 and March 2020, 12 shoulders with locked PSFD were admitted to our institution (level I trauma center). The inclusion criteria were as follows: (1) acute first-time locked PSFD, (2) underwent ORIF with osteosynthesis, (3) age >18 years, (4) signed informed consent for study participation, and (5) had ≥12 months of follow-up data available. The exclusion criteria were as follows: (1) acute first-time posterior instability event involving a subluxation without the engagement of the humeral head or spontaneous reduction, (2) recurrent dynamic posterior instability, (3) chronic static posterior glenohumeral instability with degenerative changes, and (4) irreparable fracture candidate for a prosthesis [8]. Data were collected from the pre- and postoperative registries of the study hospital. Table 1 presents the evaluated demographic characteristics.

Demographic characteristics
Intervention
All patients had an acute, locked PSFD at the time of their initial evaluation at the emergency department. Patients underwent shoulder radiography (anteroposterior and outlet views) and computed tomography (CT) imaging of the injured shoulder for initial assessment and preoperative planning. A closed reduction was not successful or was not attempted because patients had an associated proximal humeral fracture or an RHS lesion affecting >25% of the humeral head articular surface with a high risk of fracture propagation. For these reasons, ORIF with osteosynthesis was indicated in all included cases.
Surgical Technique
The procedure was performed under general anesthesia and an interscalene block with the patient in a beach chair position. A standard deltopectoral approach was used for all patients. In some cases, when open reduction was difficult, a posterior arthroscopic portal was made to insert a spatula until the humeral head was felt. The spatula was slid in close to the humeral head until contact with the posterior glenoid wall was achieved. The procedure could be performed under fluoroscopy. The humerus was internally rotated to create a gap to insert the spatula between the posterior glenoid rim and the humeral head. Once the spatula came to sit on the posterior glenoid rim, it could act as a lever, using the glenoid as a fulcrum, to push the head laterally to unlock it. Gentle external rotation was performed so that the humeral head could glide over the spatula, and the joint was reduced (Fig. 1). Then, according to preoperative imaging planning and intraoperative findings, definitive surgical treatment was performed to achieve joint reconstruction. If there was a significant RHS (>25% by McLaughlin [16]) (Fig. 2), a joint exploration of the articular surface was performed. Joint exposure was performed through the lesser tuberosity (LT) fracture or osteotomy of the LT in patients without an LT fracture (Fig. 2). Any significant articular head fragment was disimpacted, anatomically reduced, and fixed with headless cannulated compression screws (Fig. 3). If an anterior residual humeral head defect remained after disimpaction of the articular surface, it was filled with the subscapularis (SSC) tendon or medialization of the LT (modified McLaughlin [16,17]) with or without the use of complementary allograft bone chips. Fixation of the LT was performed with 3.5-mm cancellous screws or 4.75–5.5-mm titanium anchors (Fig. 4). Finally, if there was significant displacement of a greater-tuberosity fracture and/or neck fracture, a proximal humerus-locked plate was added (Fig. 4).
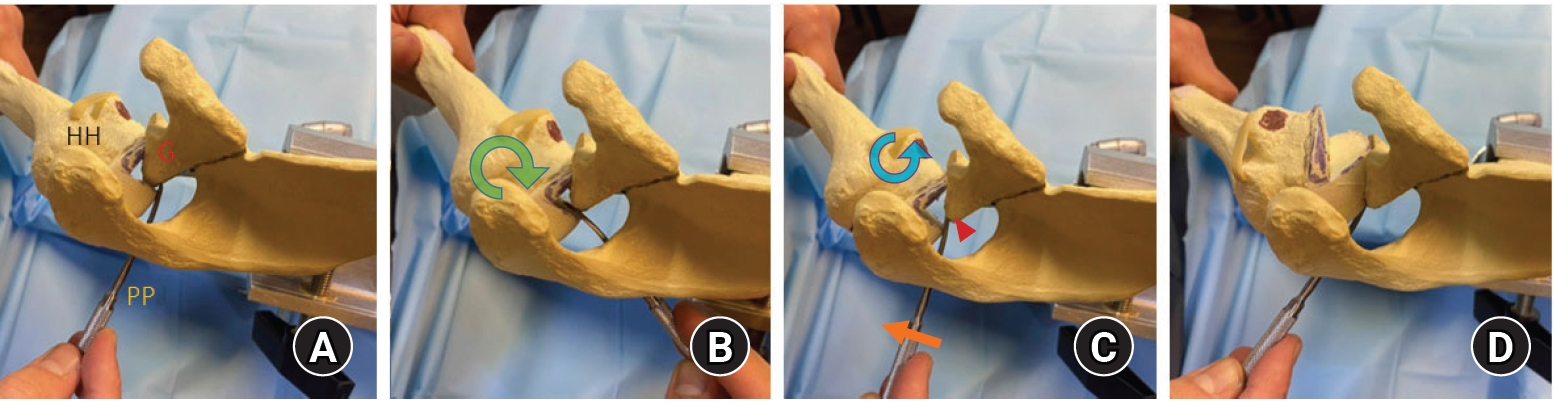
Left shoulder, superior view. (A) A classic posterior arthroscopic portal is made to allow insertion of a spatula until the humeral head (HH) is felt; then, the spatula is slid in close to the humeral cartilage until contact with the posterior glenoid (G) wall is achieved. (B) The humerus is internally rotated to create a gap to insert the spatula between the posterior glenoid rim and the HH. (C) The spatula sits on the posterior glenoid rim so that it can act as a second-class lever, using the glenoid as the fulcrum to push the head laterally while gentle external rotation is performed, so the HH can glide over the spatula. (D) The joint was reduced. Green arrow, internal rotation; blue arrow, external rotation; arrowhead, fulcrum; orange arrow, effort. PP: posterior portal.
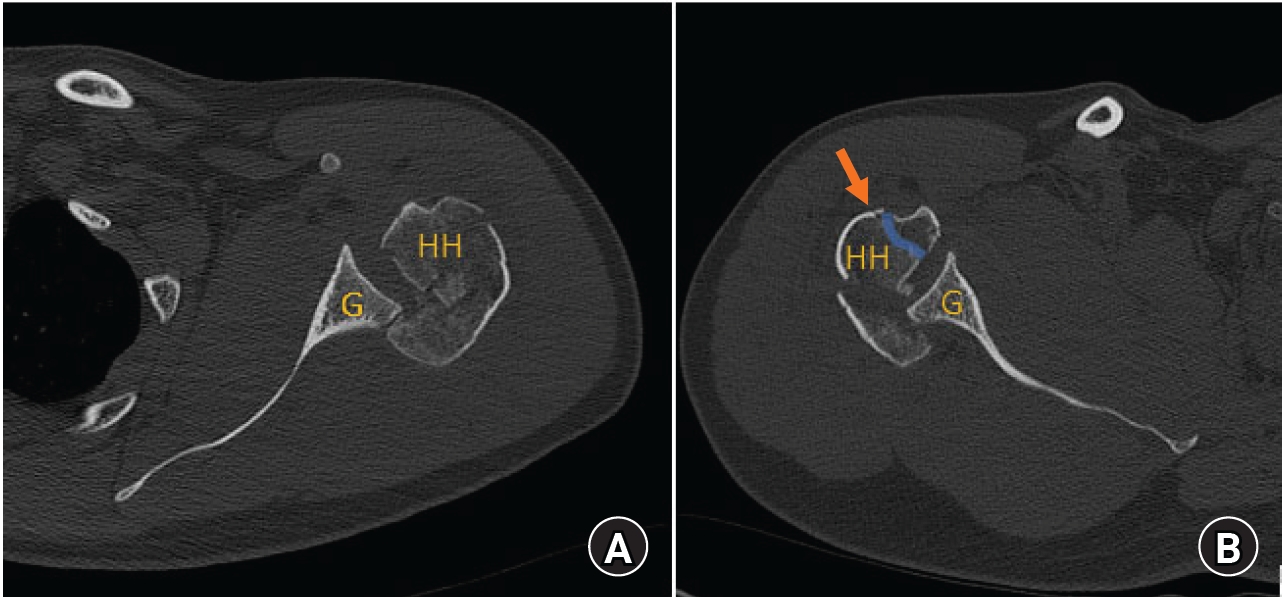
(A) Axial view of computed tomography of a left shoulder showing a posterior shoulder fracture–dislocation with significant reverse Hill-Sachs of 50%. (B) Axial view of computed tomography of a right shoulder showing the entry point for joint exploration (orange arrow) of a posterior locked dislocation when a lesser tuberosity fracture is present (blue line). HH: humeral head, G: glenoid.
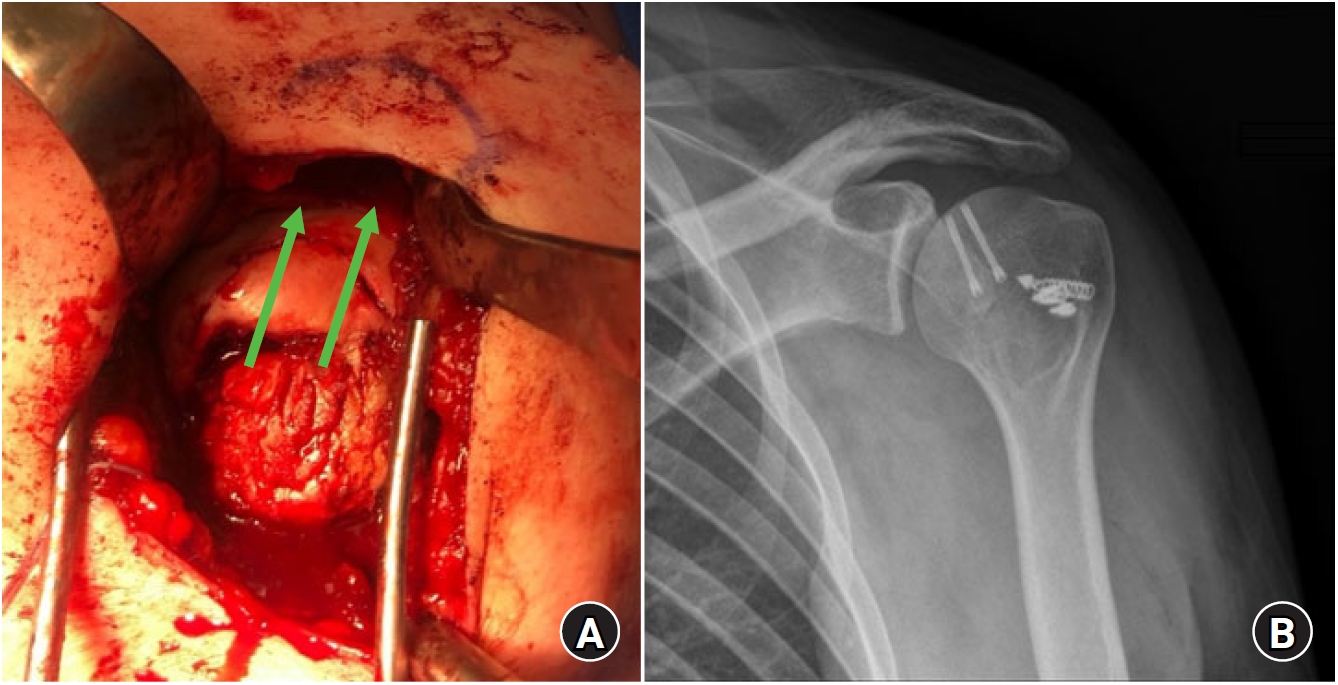
(A) Intraoperative photo of a left shoulder through a deltopectoral approach showing humeral articular surface reduction and headless screws direction (green arrows). (B) Left shoulder X-rays showing postoperative anatomical reduction and fixation.

(A) Left shoulder X-ray showing headless compression screws for articular surface reduction (green arrow), a 4.0-mm cancellous screw for modified McLaughlin fixation (orange arrow), and knotless suture anchors for subscapularis tendon reinforcement (blue arrow). (B) Left shoulder postoperative X-ray showing the use of a PHILOS (DePuy Synthes, Raynham, MA, USA) plate to fix an associated greater-tuberosity fracture on top of the articular reduction with headless cannulated screws.
After surgery, all patients were placed in a neutral-rotation shoulder-immobilization device for 4–6 weeks. Pendulum exercises were started at 2 weeks of surgery, passive mobilization was started at 4 weeks, and active exercises were started 8 weeks after surgery, respectively. There were no differences in the postoperative rehabilitation program according to the type of fracture.
Outcome Measurements
The clinical outcomes were evaluated at the end of the follow-up. We used the modified University of California, Los Angeles (UCLA) mod scoring system, American Shoulder and Elbow Surgeons (ASES) questionnaire, subjective shoulder value, and visual analog scale (VAS). Clinically, the following complications were evaluated: reluxation, postoperative neurovascular injuries, and reoperation rate. Imaging follow-up was performed using shoulder radiographs at 6 and 12 months. The variables registered were failed osteosynthesis, varus collapse, avascular necrosis (AVN), and non-union. If necessary, during follow-up, a new CT scan was requested by the surgeon. AVN of the humeral head was classified according to the system reported by Cushner and Friedman [18], and non-union was defined as a complete absence of trabecular bone formation or cortical continuity.
Statistical Analysis
Data were analyzed using the IBM SPSS ver. 25 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to verify the normal distribution of quantitative variables. The correlation between the preoperative variables (age and TFIS) and functional scores was analyzed using Pearson’s coefficient for parametric variables and Spearman’s ρ for non-parametric variables. An independent two-sample t-test was used to identify any significant mean difference in functional scores according to preoperative variables like laterality of the injury, dominant side injury, RHS, and articular bone fragment. The significance level was set at p=0.05.
RESULTS
Twelve shoulders (11 patients) were included in this study, with a mean age of 40.6 years (range, 19–62 years). The mean follow-up period was 23.3 months (range, 12–63 months). The most frequent mechanism of injury was high-energy trauma (car/motorcycle accident and fall from a height). Eleven (91.6%) patients were treated in the acute stage after the initial injury. Eight of these patients (66.7%) underwent surgery between days 0–2, and the other 4 underwent surgery on days 12, 14, 17, and 55, respectively.
Table 2 describes the patterns of injury and surgical treatment performed for each patient. Ten patients had complex PSFD. RHS injury of >25% was present in nine cases, and only 1 patient had a glenoid defect, which was found to be non-significant (<20%). At the 12-month follow-up visit, 10 patients (83.3%) completed a clinical evaluation with functional scores (Table 3).
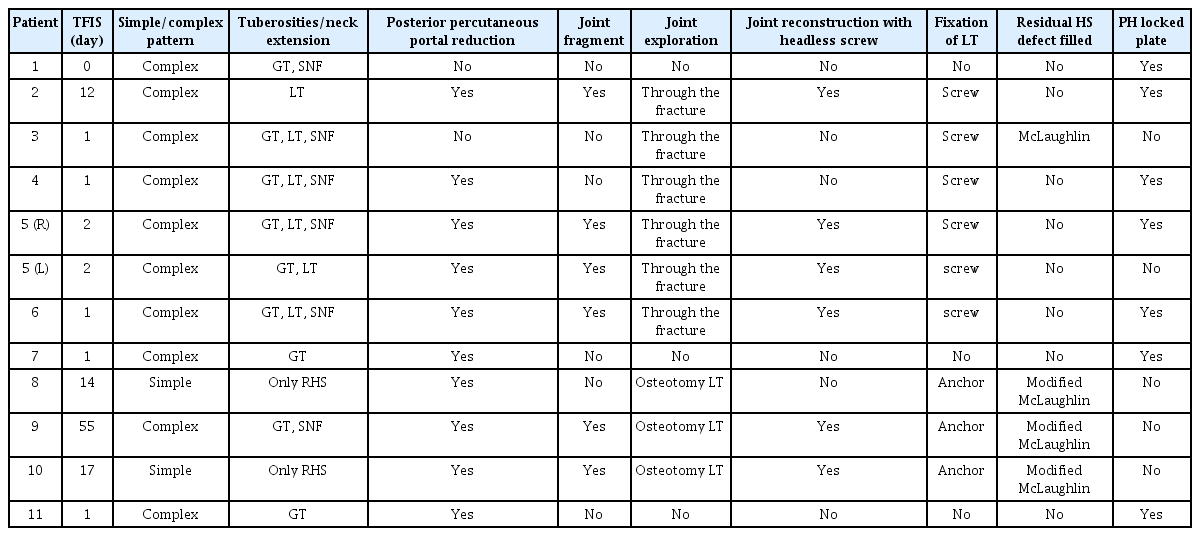
Injury patterns and surgical treatment

Functional outcomes and complications
No significant correlations were found between age, TFIS, and functional scores. Moreover, no significant mean differences were found in scores according to preoperative variables (laterality of the injury, dominant-side injury, and presence of articular bone fragments). The overall complication rate was 16.6%. One patient had post-traumatic stiffness that required plate removal and joint release, and another patient developed chronic pain that required permanent management from the chronic pain unit. No other re-interventions were performed. No cases of reluxation, hardware failure, AVN, varus collapse, non-union, or neurological or vascular injury were reported (Table 3).
DISCUSSION
The most important finding of this study was that good functional results and a low rate of complications can be achieved with open surgical treatment for locked PSFD. A correct understanding of these injuries and preoperative planning allowed us to apply an adequate surgical technique and obtain good results. There has been increasing interest in posterior shoulder dislocation in recent years. Moroder and Scheibel [8] described a new ABC classification system, including mechanism, imaging, and temporality. Our study only included patients with locked PSFD classified as A2 according to the ABC classification. Most cases were locked dislocations due to high-energy trauma and were associated with a proximal humeral fracture (complex PSFD). However, fractures associated with complex PSFD may facilitate an earlier diagnosis and treatment [7].
In a recent study by Park et al. [1], four of six patients with locked PSFD underwent ORIF, obtaining average Constant, ASES, and VAS scores of 67, 67.5, and 2 points, respectively, after a mean follow-up period of 26.2 months. In another study [3], 13 patients with locked PSFD who underwent a modified McLaughlin procedure had a mean UCLA score of 25.5 points at the end of a mean follow-up period of 12.5 months. Excellent/good results have been reported in surgical treatment of simple locked PSFD in 62%–82% of patients at mid-term follow-up [5,9]. Liu et al. [19] analyzed 18 patients with locked PSFD associated with only an LT fracture who underwent ORIF of the LT and found that a longer TFIS had a negative effect on functional scores. We were unable to demonstrate that the TFIS had a negative effect because of the limited number of participants in our study, with only one patient being treated surgically as a chronic case. Finally, excellent functional results were published by Banerjee et al. [20], who studied seven patients with acute locked PSFD who underwent a modified McLaughlin procedure, obtaining average Constant and ASES scores of 92 and 98 points, respectively. Their good results could be linked to the exclusion of patients with associated proximal humerus fractures and those surgically treated 2 weeks after the initial trauma. As seen in our study, a modified McLaughlin technique is widely used to fill RHS injuries of 20%–40% of the humeral head. We added headless compression screws to fix the disimpacted head bone fragments to ensure absolute stability of the articular fracture and favor the viability of cartilage and subchondral bone. Therefore, the functional results in our study are similar to those of other investigations in the literature.
Until the end of the follow-up period, no case of AVN or bone collapse had been reported. One reason could be that not all patients had enough follow-up, and we did not enroll any patients with 4-part fractures. However, due to AVN occurring mostly in acute cases [7], we cannot attribute our low rate of AVN to temporality because most of our patients were operated on in the acute stage.
The complication rate has varied considerably in previously published studies. AVN has been reported in 0%–50% of cases after surgical treatment at mid-term follow-up [1,3,18,19,21]. Basal et al. [7] published a systematic review on complication rates in 228 patients. An overall complication rate of 15.3% was found, similar to our results, with worse outcomes recorded in chronic cases (23% chronic vs. 8.8% acute). The most frequent complication was AVN (3.5%), and six out of eight cases occurred in patients treated with early surgery.
To date, there are no clear risk factors for AVN in surgically treated patients after PSFD. Further studies are needed to understand whether temporality, initial trauma energy, associated fractures, or type of ORIF are associated risk factors for AVN. As seen in most of the reported case series, no recurrent dislocations occurred during follow-up. This was probably because most of the reconstruction techniques used to treat RHS are sufficient to prevent recurrent glenohumeral instability [4,11,22].
Preoperative image analysis was essential for surgical planning. Understanding fracture patterns and humeral head anterior defects allows us to make a standardized recommendation for future cases. Thus, our main recommendations are as follows. First, use a posterior glenohumeral percutaneous portal to assist joint reduction with a spatula if reduction is difficult, regardless of the type of fracture; this can significantly reduce surgical time. Second, identify the presence of an impacted head articular fragment or significant RHS (>25%); if present on preoperative CT images, it will be necessary to explore the joint. Third, joint exploration can be performed by SSC tenotomy or peeling, osteotomy of the LT, or through the LT fracture. Identify any LT fracture on preoperative CT images to avoid unnecessary SSC tenotomy or peeling. In cases where there is no LT fracture, an LT osteotomy could have advantages over peeling or tenotomy of the SSC tendon; this avoids iatrogenic disinsertion of the SSC tendon, allows filling of RHS when it is not possible to reconstruct the joint surface, or it can be used as subchondral support for the reconstructed head joint fragment by medializing the LT. Fourth, always attempt anatomical reconstruction of the articular surface. To do this, elevate fragments, seek anatomical reduction, and add headless cannulated compression screws in large unstable fragments to achieve absolute stability. Fifth, always reinsert the SSC tendon or fix the LT. Any residual anterior joint defect can be filled with the modified McLaughlin procedure or using the SSC tendon. Sixth, in the presence of a greater tuberosity or neck fracture, add a locked proximal humerus plate. These recommendations could aid in decision-making and decrease the surgical time (Fig. 5). Finally, the use of large auto/allografts, rotational osteotomies, or arthroplasties was not necessary. All our cases had <50% of the articular surface compromised, and most underwent early surgery. This allowed the joint surface to be reconstructed in all cases, reducing the final size of the head defect to <25% of the humeral head articular surface.
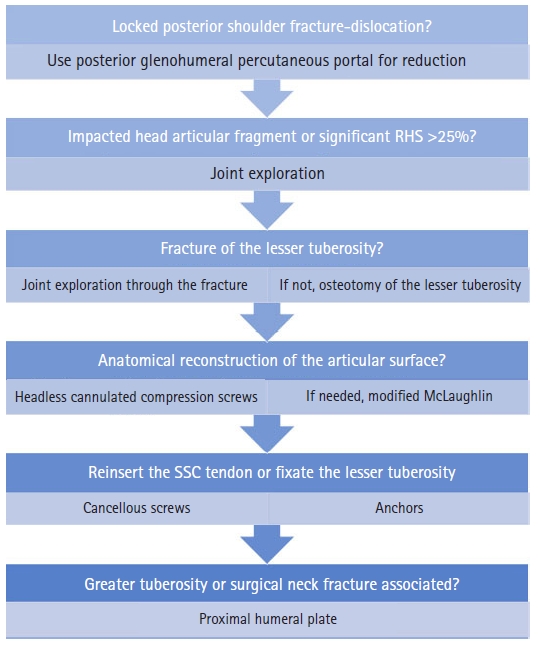
Decision-making for the treatment of locked posterior shoulder fracture–dislocation. RHS: reverse Hill-Sachs, SSC: subscapularis.
This study has some limitations. The low frequency of a locked PSFD contributed to our small sample size and retrospective study design. Other limitations include a lack of a control group, a heterogeneous sample of patients, and multiple surgeons being involved in the treatment despite the standardized approach. Lastly, the clinical outcomes may differ from those of other studies because all our patients were under workers’ compensation insurance, which has been described as a prognostic factor for poorer results in other shoulder injuries [23]. Larger comparative controlled studies should be conducted to evaluate functional and prognostic results in the treatment of patients with a locked PSFD.
Open surgical treatment of locked PSFD can achieve good functional results. Correct understanding of these injuries and preoperative planning helped us to achieve a low rate of complications like AVN and re-interventions. Further comparative controlled studies are needed to understand whether temporality, initial trauma energy, associated fractures, and type of ORIF are associated risk factors for complications and functional results.
Notes
Financial support
None.
Conflict of interest
None.