Postoperative clinical outcomes and radiological healing according to deep and superficial layer detachment in first facet involving subscapularis tendon tear
Article information

Abstract
Background
Subscapularis tendon insertion at the first facet has separate layers (deep and superficial). The purpose of this study is to evaluate postoperative clinical outcomes and radiological healing according to each layer of detachment in the first facet involving subscapularis tendon tear.
Methods
Eighty-three patients who underwent arthroscopic repair due to First facet involving the scapularis tendon tear accompanying small to medium sized posterosuperior cuff tear were classified into three groups (group A: deep layer partial detachment, group B: deep layer complete detachment, but no superficial layer detachment, and group C: deep layer and superficial layer complete detachment). Subscapularis tendon healing was evaluated using computed tomography arthrogram and clinical result was evaluated using American Shoulder and Elbow Surgeons (ASES) shoulder score, Constant score and University of California Los Angeles (UCLA) shoulder score.
Results
Retear rate of the subscapularis tendon was 2.2%, 18.2%, and 33.3% in group A, group B, and group C, respectively. These rates showed statistically significant difference among the three groups, which were classified by deep and superficial layer detachment in the first facet (p=0.003). Group A showed significant difference in subscapularis tendon healing compared with group B and group C (p=0.018 and p<0.001, respectively), but there was no statistical difference between group B and group C (p=0.292). Regarding clinical outcomes, there was no significant difference among three groups in ASES and UCLA score at final follow-up (p=0.070 and p=0.106, respectively).
Conclusions
Complete detachment of deep layer may be related with retear occurrence regardless with detachment of superficial layer, but clinical outcome may not be related with each layer detachment in the first facet involving subscapularis tendon tear.
INTRODUCTION
The subscapularis, located at the front of the glenohumeral joint, is the largest muscle in the rotator cuff [1]. Gleason et al. [2] reported that in radiological, anatomical, and histological studies, the fibers of the subscapularis tendon have been shown to cross the bicipital groove and connect to the coracohumeral ligament and the supraspinatus tendon. Studies about subscapularis tendon insertion areas have reported that the superficial layer of the subscapularis tendon continues over the biceps tendon and inserts into the greater tuberosity, whereas the deep layer of the subscapularis tendon inserts into the lesser tuberosity just medial to the long head of the biceps tendon [2-5]. These separate layers and insertions are more distinct in the upper portion of the subscapularis tendon than that in the lower portion, with the muscular portion directly inserting into the bone. Most previous studies on subscapularis tendon tears have focused on lesser tuberosity, that is, partial and complete tears according to the degree of detachment from the lesser tuberosity [5-10], but they have not evaluated subscapularis tendon tears according to each layer (deep and superficial layer) of detachment. Moreover, there is no postoperative clinical and radiological healing study comparing the three possible tear types according to each layer (deep and superficial layer) of detachment in the first facet: (1) partially detached deep layer and intact superficial layer, (2) completely detached deep layer and intact superficial layer, and (3) completely detached deep layer and completely detached superficial layer. This study aimed to evaluate postoperative clinical outcomes and radiological healing according to each layer of detachment in the first facet involving subscapularis tendon tear.
METHODS
This study was approved by Inje University Busan Paik Hospital (IRB No. BPIRB 2021-09-008-001). Informed consent was confirmed by the IRB as unnecessary papers.
Participant Selection
After approval from the institutional review board, the corresponding author in this paper evaluated all the patients who underwent arthroscopic rotator cuff repair between March 2013 and February 2016. Patients who underwent (1) repair due to small- to medium-sized rotator cuff tears (RCTs), (2) repair for concomitant subscapularis tendon tear, (3) computed tomogram arthrogram (CTA) at 6 months postoperatively, and (4) at least 2 years of follow-up were included. The exclusion criteria were as follows: (1) osteoarthritis or cuff tear arthropathy, (2) previous fracture, dislocation, or operation history at the ipsilateral shoulder, (3) repair due to retear, and (4) magnetic resonance imaging (MRI) performed in another institution. Among the 314 patients who underwent arthroscopic rotator cuff repair from March 2013 to February 2016, 142 patients underwent arthroscopic rotator cuff repair due to small- to medium-sized tears with concomitant subscapularis tendon tears. Among the 142 patients, 106 underwent CTA at 6 months postoperatively and 83 patients participated in at least two years of follow-up. After applying the exclusion criteria, 83 patients were selected as final participants (Fig. 1).

Flowchart of the study. Group A: deep layer partial detachment, Group B: deep layer complete detachment but no superficial layer detachment, Group C: deep layer and superficial layer complete detachment.
Evaluation of Subscapularis Tendon Tear Using MRI
We evaluated subscapularis tendon tear using axial and sagittal oblique views of MRI [11-13]. First, after choosing the sagittal oblique view series, we traced the image medially from the biceps tendon on the bicipital groove and selected the most lateral image slice of the first facet and named it the sagittal oblique view of the facet (SOVfacet). Second, “the scout function” was activated with a reference image as the SOVfacet, and then, the axial view series was chosen. Axial images were selected over the first facet of the lesser tuberosity and named it as the axial view of the facet (AVfacet) (Fig. 2). Using SOVfacet, the craniocaudal detachment of the deep layer of subscapularis tendon from the first facet was evaluated. A “deep layer partial detachment” was defined as a tear that showed some remaining tendon attached to the first facet in the SOVfacet, and a “deep layer complete detachment” was defined as a tear that showed no remaining tendon attached to the first facet in the SOVfacet. Using the AVfacet, detachment of the superficial layer of the subscapularis tendon was evaluated over the intertubercular groove and lesser tuberosity. “No superficial layer detachment” was defined when the tendon displayed continuity over the lesser tuberosity of the intertubercular groove in the AVfacet, and “superficial layer complete detachment” was defined when the tendon did not show continuity over both the lesser tuberosity and intertubercular groove in the AVfacet. Using sagittal oblique and axial views, subscapularis tear patients were classified into three groups (group A: deep layer partial detachment, group B: deep layer complete detachment, but no superficial layer detachment, and group C: deep layer and superficial layer complete detachment) (Fig. 3).

Determining subscapularis tendon tear with magnetic resonance imaging using sagittal oblique view of the facet (SOVfacet) and axial view of the facet. Check the first facet in the axial image (A), and select the SOVfacet (B), which is the image corresponding to the most lateral image of the first facet. Trace the image proximal (D), middle (E), and distal (F) portion of the first facet to evaluate the detachment of superficial layer using the scout function in the selected SOVfacet image (C). Asterisk indicates, first facet of LT; black arrow, most medial aspect of first facet; white arrowhead, most lateral aspect of first facet. The red line in (A) indicates the sagittal plane corresponding to (B) and the three red lines in (C) represent the axial planes corresponding to images D, E, and F from the top.
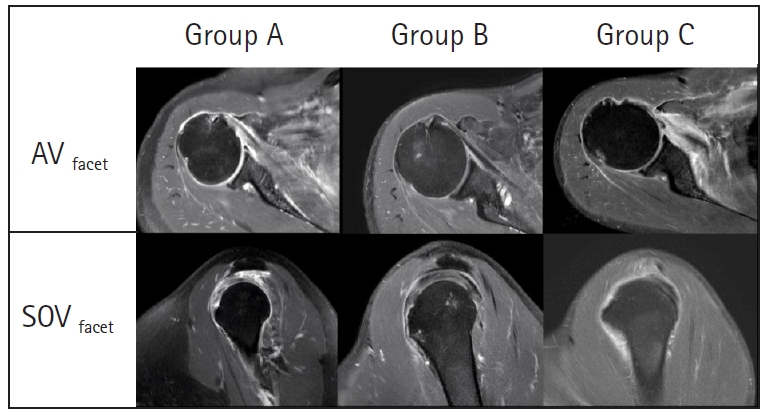
Evaluation of subscapularis tendon tear using magnetic resonance imaging. Axial view of the facet (AVfacet) of group A (deep layer partial detachment) (A), group B (deep layer complete detachment but no superficial layer detachment) (B), and group C (deep layer and superficial layer complete detachment) (C). Sagittal view of the facet (SOVface) of group A (D), group B (E), and group C (F).
Clinical Evaluation
Interviews, questionnaire surveys, and physical examinations were performed a day before the surgery and at the last follow-up. The subjective level of pain was measured using a visual analog scale (VAS). The range of motion (was measured. Scapular plane abduction, external rotation at the side, and internal rotation behind the back were measured. For statistical analysis, the spinal segment was converted into numbers—segments T1–T12 were designated as 1–12, segments L1–L5 as 13–17, and the sacrum as 18. Muscle strength was measured using a handheld dynamometer, Nottingham Mecmesin Myometer (Mecmesin Co., Nottingham, UK). Clinical scores were evaluated using the American Shoulder and Elbow Surgeons (ASES) shoulder score, Constant score, and University of California Los Angeles (UCLA) shoulder score.
Radiological Evaluation
Using preoperative shoulder MRI, additional data regarding tear size, degrees of tear, and fatty degeneration of the rotator cuff were evaluated. To evaluate the degenerative state of the subscapularis tendon, the degree of fatty degeneration of the rotator cuff was evaluated using the modified Goutallier classification [14]. Cuff healing was evaluated using a CTA that was taken 6 months after surgery. We evaluated tendon healing for overall healing (complete healing and partial healing defect) and retear [15]. (Fig. 4)

Degree of subscapularis tendon healing after repair. (A) Complete healing of the subscapularis. The continuity of the subscapularis is fully maintained. (B) Partial healing defect of the subscapularis. The continuity of the subscapularis is cut off in some images, but there is no full thickness tear. (C) Retear of the subscapularis. The continuity of the subscapularis is fully cut off by a full thickness tear.
Surgical Method
All arthroscopic procedures were performed by a single surgeon (JHK) with the patient in a beach chair position [16-18]. Under general anesthesia, three routine arthroscopic portals (anterior, posterior, and lateral) were made. After the arthroscopic examinations and evaluation of the intra-articular structure, the intra-articular side of the subscapularis was evaluated using a 70° arthroscope. The subacromial space was then accessed, confirming RCTs, reparability, and features of the RCTs including the bursal side of the subscapularis. Further, the subscapularis tendon tear of the lesser tuberosity footprint was repaired using the single-row repair technique in the intra-articular space. Posterosuperior cuff repair was performed using the suture bridge technique in the subacromial space. Further, the accompanying biceps lesions were treated by two methods. Biceps tenodesis was performed in relatively young and active patients, and tenotomy was performed in less active or elderly patients.
Statistical Analysis
All statistical analyses were performed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA). The Student t-test was used to analyze continuous variables, and the Mann-Whitney U-test was used to analyze data with non-normal distributions. Categorical variables were analyzed by using the chi-square or Fisher exact tests. The one-way analysis of variance (ANOVA) test was used to perform comparisons of subgroups. If the one-way ANOVA test indicated a significant difference, the Bonferroni method and post-hoc test were used. All tests were analyzed with a 95% confidence level. The level of significance was set at 0.05.
RESULTS
Eighty-three patients (34 men and 49 women) were included in the final analysis. The mean patient age was 60.67±6.66 years. Patient demographics according to groups are summarized in Table 1.

Demographic data according to groups
Tear Characteristics According to Groups
The mean subscapularis tendon superoinferior tear size were 6.37±2.56 mm, 15.00±2.09 mm, and 17.07±3.84 mm in group A, group B, and group C, respectively (p<0.001). The mean fatty degeneration of subscapularis was 0.13±0.40, 1.32±0.82, and 1.80±1.08 in group A, group B, and group C, respectively (p<0.001). There were statistically significant differences in the degree of biceps tear and dislocation among three groups (p<0.001 and p<0.001, respectively). All the values like subscapularis tendon superoinferior tear size, fatty degeneration of subscapularis, and the degree of biceps lesion show statistically significant differences among these groups (Table 2).
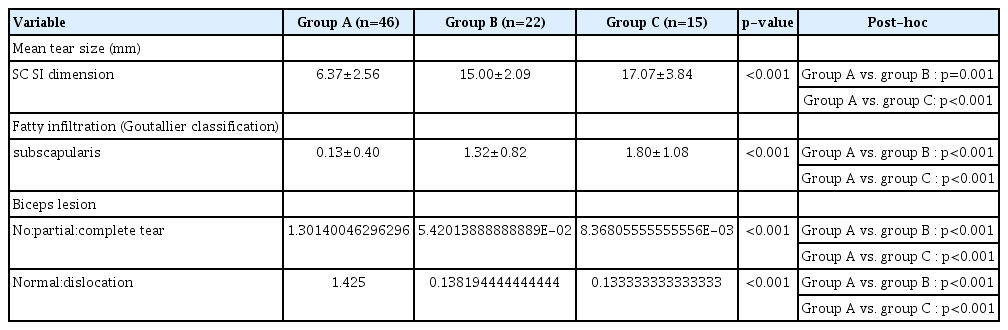
Tear characteristics according to groups
Radiological Healing According to Groups
The radiological healing according to groups is summarized in Fig. 5. There were statistically significant differences in subscapularis tendon healing among three groups (p=0.039). In post-hoc analysis, group A showed statistically significant difference in subscapularis tendon healing compared with group B and group C (p=0.018 and p<0.001, respectively), but there was no statistical difference between group B and group C (p=0.292) (Fig. 5).

Structural healing rate of subscapularis tendon after repair among three groups. Group A: deep layer partial detachment, Group B: deep layer complete detachment but no superficial layer detachment, Group C: deep layer and superficial layer complete detachment. *Comparison of three groups; †Post-hoc analysis each groups.
Clinical Outcomes According to Groups
At final follow-up, the VAS, ASES, UCLA shoulder, and Constant scores improved statistically in all three groups compared to those in the preoperative period (p<0.001). However, there was no significant difference among three groups in VAS, ASES, and UCLA score at final follow-up (p=0.059, p=0.070 and p=0.106, respectively). More details are shown in Table 3.

Clinical outcomes according to groups
DISCUSSION
In the current study, the subscapularis tendon healing rate after surgery showed statistically significant difference among three groups according to deep and superficial layer detachment in the first facet (p=0.003). However, there was no significant difference among three groups in ASES and UCLA score at final follow-up (p=0.070 and p=0.106, respectively).
With regard to subscapularis tendon healing, there was 2.2% retear and 97.8% healing rate in group A (deep layer partial detachment), 18.2% retear and 81.8% healing rate in group B (deep layer complete detachment, but no superficial layer detachment), and 33.3% retear and 66.7% healing rate in group C (deep layer and superficial layer complete detachment). Group A showed statistically significant difference in subscapularis tendon healing compared with group B and group C (p=0.018 and p<0.001, respectively), but there was no statistical difference between group B and group C (p=0.292). Although the cause of these differences of tendon healing rates among the three groups cannot be clearly elucidated in the current study, two possible reasons were speculated. First, group B and group C showed more degenerative changes in the subscapularis muscle than group A from the point of mean fatty degeneration. These changes could lower the healing rate after subscapularis repair. Second, it may be a problem of tension in repairing the retracted layer of subscapularis tendon in groups B and C during surgery. According to a study by Meyer et al. [19], when partial tear of the subscapularis occurs, shortening of the musculotendinous unit and extension of the tendon due to retraction occur. Therefore, in subscapularis tears, over-tension or insufficient tension could be observed during surgery due to the extension of these tendons. In our study, in the case of group A, all the tears were Yoo IIB and slightly retracted partial tears. In case of group B (deep layer complete detachment, but no superficial layer detachment), it was difficult to clearly identify the most lateral side of the retracted deep layer of the subscapularis tendon. Moreover, since the suture was performed in the intra-articular space using an arthroscope, there was a possibility of tension mismatch between the superficial layer and deep layer. In the case of group C (deep layer and superficial layer complete detachment), even though most of the lateral side of the retracted tendon layer was easily identified, restoration of the retracted tendon may cause over-tension. It was speculated that these factors may contribute to the higher retear rate compared with group A (deep layer partial detachment).
With regard to clinical outcomes, in the current study, three groups showed no significant difference at final follow-up. This finding implies that first facet involving subscapularis tear does not affect the clinical outcomes. The Constant scores at final follow-up were 78.3±9.6 in group A, 70.2±17.2 in group B, and 71.6±9.6 in group C. Although there was a statistically significant difference in the Constant scores among three groups, these differences might not be clinically significant. The healing after repair of the subscapularis tendon tear has been known to be an important factor in clinical outcomes. Shibayama et al. [14] reported that there was a difference in clinical results between the subscapularis-healed group and the retear group after performing arthroscopic subscapularis suture bridge repair. Kim et al. [15] and Park et al. [20] also reported that in subscapularis tears associated with large-to-massive posterosuperior RCTs, healing of the subscapularis affects clinical outcome. However, in our study, the three groups showed significant differences in radiological healing rate, but showed no clinical difference. The cause of this finding cannot be clearly defined in the current study, but we assumed that the following three factors of our study design might lead to no clinical difference despite difference of subscapularis healing rate among three groups; (1) all the subscapularis tendon tears were limited to first facet and (2) posterosuperior cuff tears were small to medium size. However, the high retear rates of subscapularis tendon after repair in group B and group C could worsen the clinical outcomes in long-term follow-up. Therefore, surgeons should interpret our result with caution.
This study has some limitations. First, as this was a retrospective study, it was difficult to exclude selection bias in the selection of patient groups, and it is thought that selection bias may act as a confounding variable. Second, the degree of the subscapularis tendon tear was limited to the first facet. Therefore, cases in which the subscapularis tendon tear exceeded the first facet were excluded; hence, not all subscapularis tendon tears were included. However, in the case of tears exceeding the first facet, studies have shown that the subscapularis tendon tear itself is a factor affecting the postoperative outcome [20-22]. Because we wanted to evaluate postoperative clinical outcomes and radiological healing according to each layer detachment, the size of the subscapularis tear, which could be another confounding factor, was unified. Finally, the treatment for the biceps tendon lesion was not the same. Biceps tenodesis was performed in young patients, and tenotomy was performed in less active or elderly patients. The fact that the same procedure was not performed in all patients could also act as a confounding variable [23-26].
Although clinical outcome may not be related with each layer detachment in first facet involving tear, considering the lower healing and higher retear rate after subscapularis repair in group B and group C compared with group A, complete detachment of the deep layer may be related with retear risk regardless with detachment of superficial layer. Therefore, in repairing subscapularis tendon tear, surgeons should carefully evaluate the degree of deep layer detachment without overlooking this lesion. Further, they should make efforts to clearly identify the tear pattern and margin of this deep layer detachment using a 70° arthroscope.
Notes
Financial support
None.
Conflict of interest
None.