Mid-term Clinical and Radiological Outcomes of Latissimus Dorsi Tendon Transfer in Massive Rotator Cuff Tears
Article information

Abstract
Background
This retrospective study was undertaken to evaluate mid-term clinical and radiological outcomes of lattisimus dorsi (LD) tendon transfer in patients with irreparable massive rotator cuff tears (MRCT). We hypothesize that LD tendon transfer would provide safe and satisfactory clinical outcomes at mid-term follow-up.
Methods
From November 2008 to December 2016, 23 patients (57.5 ± 4.4 years; 20 male, 3 female) who underwent LD tendon transfer for massive tears, were enrolled. Inclusion criteria were irreparable MRCT. Exclusion criteria included full thickness subscapularis tear, rotator cuff arthropathy, anterosuperior rotator cuff tear, and osteoarthritis. Mean follow-up period was 4.7 ± 4.0 years (range, 2–12 years). Clinical assessment (American Shoulder and Elbow Surgeons [ASES], University of California, Los Angeles [UCLA], Simple Shoulder Test [SST]) and radiographic assessment (osteoarthritis [OA], acromiohumeral distance [AHI]) were evaluated.
Results
ASES, UCLA and SST scores, and range of motion (ROM), except internal rotation, improved significantly at the last follow-up (p<0.05). Also, AHI was significantly improved at the last follow-up, from 6.6 mm to 8.2 mm (p=0.008). At the final follow-up, the radiologic stages of the glenohumeral osteoarthritis were determined as stage 1 in 9 patients, stage 2 in 10 patients, stage 3 in 2 patients, and stage 4 in 2 patients. Complications were observed in 21.7% cases: 3 re-tears and 2 infections were noted in our study.
Conclusions
LD tendon transfer for irreparable MRCT provides satisfactory clinical outcomes at mid-term follow-up. Mild degenerative osteoarthritis (stage 1, 2) of the shoulder joint are common at the mid-term follow-up. Also, complications such as tear, infection should be considered.
Introduction
In massive irreparable rotator cuff tears, several treatment options include arthroscopic debridement, partial repair [1-3], superior capsular reconstruction (SCR) [4-6], auto- or allograft interposition [7], balloon spacer arthroplasty [8-10], trapezius transfer, and latissimus dorsi (LD) transfer [11] or reverse total shoulder arthroplasty (RTSA) [12-15].
Arthroscopic debridement provides pain relief by removing the damaged torn rotator cuff tissue. In partial repair, an attempt is made to repair as much cuff as possible. This partial repair generally provides good early clinical outcomes, but has shown a significantly high failure rate [1-3]. Graft interposition repair is achieved by using an acellular dermal matrix (ADM) inserted into the gap between torn retracted tendons and the greater tuberosity [7]. Several xeno- and allograft tissues including porcine or human dermis are available, and have shown promising results in some patients. Balloon spacer arthroplasty has recently been proposed, and acts by preventing humeral head migration by placing a biodegradable saline-filled spacer between the humeral head and acromion; however, there is no long-term follow-up study to determine the outcome [8-10]. Also, RTSA is very effective for irreparable rotator cuff tears in elderly patients [12-15], but due to the questionable longevity of RTSA and limited treatment options after failure, this procedure is not an ideal option for young, active patients. In the future, long term follow-up studies that compare different treatment modalities are required, to verify the superiority of a specific procedure and to determine patient specific indications.
In the massive irreparable rotator cuff tears, loss of active forward flexion and external rotation are the common principal complaints. LD transfer to greater tuberosity is capable of restoring active forward flexion and external rotation. Long term clinical outcomes are also available for LD transfer, and it is one of the useful procedures available for young and active patients. Furthermore, LD transfer has been reported for irreparable subscapularis tendon tears [16].
This study was undertaken to evaluate the clinical and radiological outcomes of LD transfer in patients with massive irreparable rotator cuff tears. We hypothesize that this procedure will provide safe and satisfactory clinical outcomes at the mid-term follow-up period, without the occurrence of definite osteoarthritis.
Methods
From November 2008 to December 2016, 25 patients underwent LD transfer for massive irreparable rotator cuff tears. Of these, 2 patients were not available for a 2-year follow-up. Finally, 23 patients were enrolled in this study. All surgeries were performed by a single surgeon.
The physical examination evaluated for range of motion (ROM), drop arm sign and hornblower’s sign. Preoperative Xrays were examined for the presence of osteoarthritis, and preoperative magnetic resonance images (MRIs) were evaluated for tendon retraction, tear size, muscle atrophy, and fatty degeneration of the torn cuff tendon (Fig. 1). Based on these factors, we predicted the repairability of these massive rotator cuff tears, and resolved whether or not to perform LD tendon transfer. The inclusion criterion was massive irreparable posterosuperior cuff tear. Exclusion criteria included combined full thickness subscapularis tendon tears, rotator cuff arthropathy, anterosuperior rotator cuff tears including full thickness subscapularis tendon tears, osteoarthritis, and patients who had undergone prior shoulder surgery on the same shoulder (Table 1).
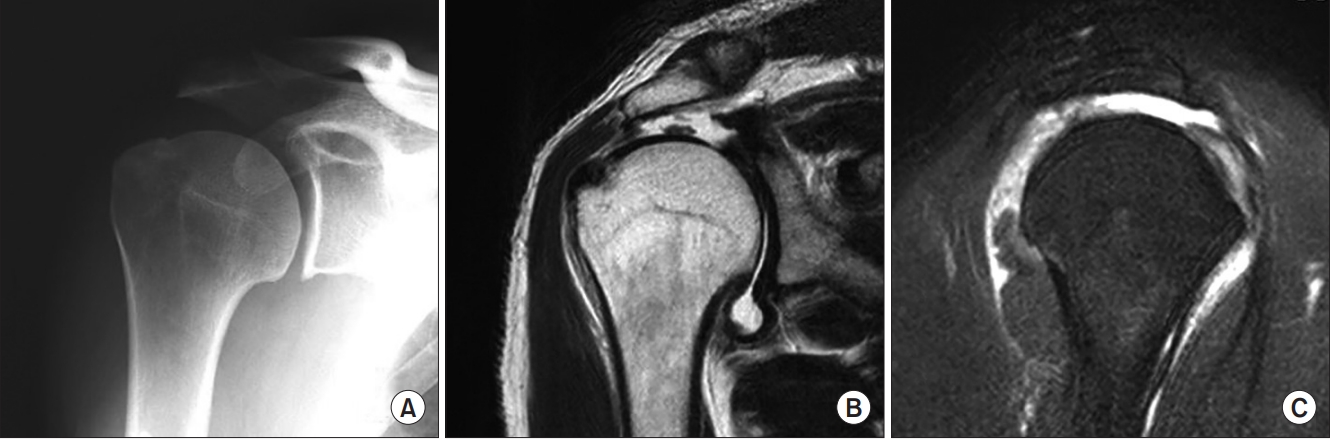
A 59-year-old male patient suffered from chronic shoulder pain due to a slip down injury. (A) Preoperative X-ray shows no definite abnormality. (B, C) Coronal and sagittal magnetic resonance imaging view show massive retracted rotator cuff tear without osteoarthritis.

Patient Demographics
Surgical Procedure
Arthroscopy was initially performed in the lateral decubitus position to check repairability of the cuff and glenohumeral arthritis. If preoperative MRI showed clearly massive retracted irreparable rotator cuff tear without arthritis, LD transfer was achieved without arthroscopic examination. However, if the preoperative MRI gave no clear indication, we first performed arthroscopy, checked for repairability of the cuff, and subsequently performed the LD transfer only for irreparable cases. Briefly, two incisions were placed on the lateral decubitus position; the first incision was placed on the lateral axillary fold. A curvilinear longitudinal incision (15 cm) was then made from the tip of the scapular to the axillary fold. After fascial incision and identifying LD, the tendinous portion of the LD tendon was released from the teres major and anterior chest wall. Using a no. 15 Knife, this tendinous portion was detached from the humeral bone (Fig. 2A). It is important to note that when performing LD tendon transfer, it is critical to maximize the respective muscle excursion (Fig. 2B) and anchor the tendon on the anterior aspect of the greater tuberosity with the arm in external rotation.
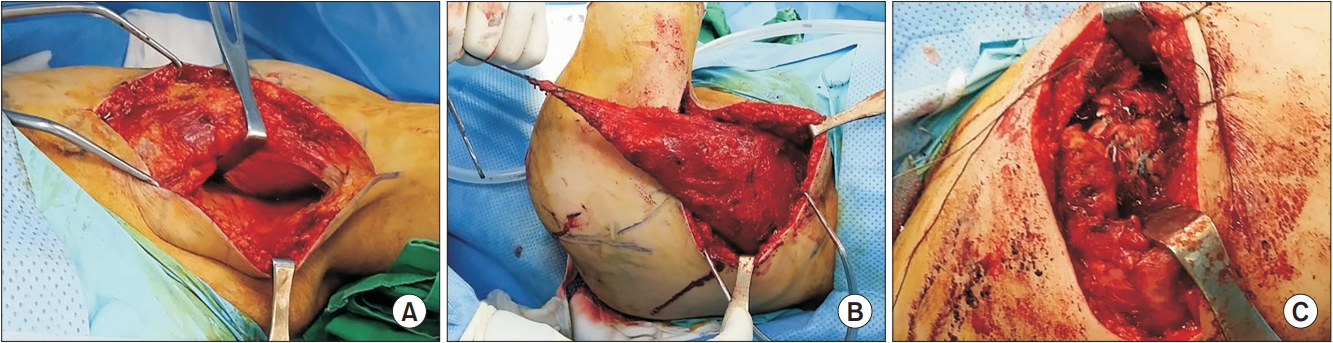
Surgical procedure. (A, B) Curvilinear longitudinal incision (15 cm) was performed from the tip of the scapular and axillary fold. After fascial incision, thin tendinous portion of the LD tendon was released and detached from the humeral bone. (C) On the anterior greater tuberosity, two anchors were inserted, after which the suture bridge rotator cuff repair was performed.
Another longitudinal 10 cm incision was made at the apex of the shoulder. The greater tuberosity was exposed after periosteal detachment of the middle deltoid. Complete removal of subacromial bursa was done, followed by decortication of the tuberosity bone. After submuscular tunneling, the tendinous portion of LD tendon was transferred to the tuberosity. Two anchors were inserted at the anterior greater tuberosity, with subsequent suture bridge repair of the transferred LD tendon (Fig. 2C). After tight repair of the transferred LD tendon, a tight repair of the middle deltoid to the lateral acromion was completed.
An abduction brace was applied during the subsequent postoperative 6 weeks, and gentle passive ROM, such as pendulum exercise, were permitted. After 6 weeks, use of the abduction brace was discontinued, and patients underwent rehabilitation by a specialized physical therapist. Active assisted exercises were initiated after 10 weeks, with subsequent introduction of progressive strengthening exercise after 3 months.
At the final follow-up, the clinical assessments (American Shoulder and Elbow Surgeons [ASES], University of California, Los Angeles [UCLA] and Simple Shoulder Test [SST] score, and ROM) and radiographic assessment using postoperative followup X-ray and MRI were evaluated. Postoperative follow-up MRI evaluated the continuity of the transferred LD tendon to the tuberosity (Fig. 2). Also, the final follow-up X-ray evaluated and compared the AHI and progression of osteoarthritis. Radiologic stages of glenohumeral arthritis, as classified by Franceschi et al. [17], were determined as follows: stage 1 (exostosis <3 mm), stage 2 (exostosis 3–7 mm with slight irregularity), stage 3 (exostosis >7 mm with joint space narrowing), stage 4 (complete loss of glenohumeral joint space).
Statistics
All data management and statistical analysis were performed using the IBM SPSS ver. 20.0 software (IBM Corp., Armonk, NY, USA). Independent t-tests were used for continuous variables. Pearson chi-squared test or Fisher’s exact test was applied to analyze the categorical variables. The level of significance was set at p<0.05.
Results
Totally, 23 patients were enrolled in our study. Mean age at surgery was 57.5 years (range, 50–67 years). There were 20 males and 3 females. The mean follow-up period was 4.7 ± 4.01 years (range, 2–12 years). Pre-operatively, all patients demonstrated positive dropping and hornblower’s sign.
The average Subjective Shoulder Value was 74% at the last follow-up. Clinical outcomes such as ASES, UCLA and SST score, and all ROM (excluding internal rotation at back) were significantly improved (p<0.05; Table 2).

Clinical Outcomes of Latissimus Dorsi Tendon Transfer at the Last Follow-up
Radiologic evaluations revealed significant change between the preoperative and postoperative AHI, from 6.6 mm to 8.2 mm, respectively (p=0.008) (Fig. 3). Compared to the preoperative X-ray, all cases showed humeral head re-centering in the immediate postoperative X-ray. Postoperative follow-up sagittal and coronal MRI images showed transferred LD tendon to the tuberosity (Fig. 4). At the final follow-up, radiologic stages of the glenohumeral arthritis were determined to be stage 1 in 9 patients, stage 2 in 10 patients, stage 3 in 2 patients, and stage 4 in 2 patients.
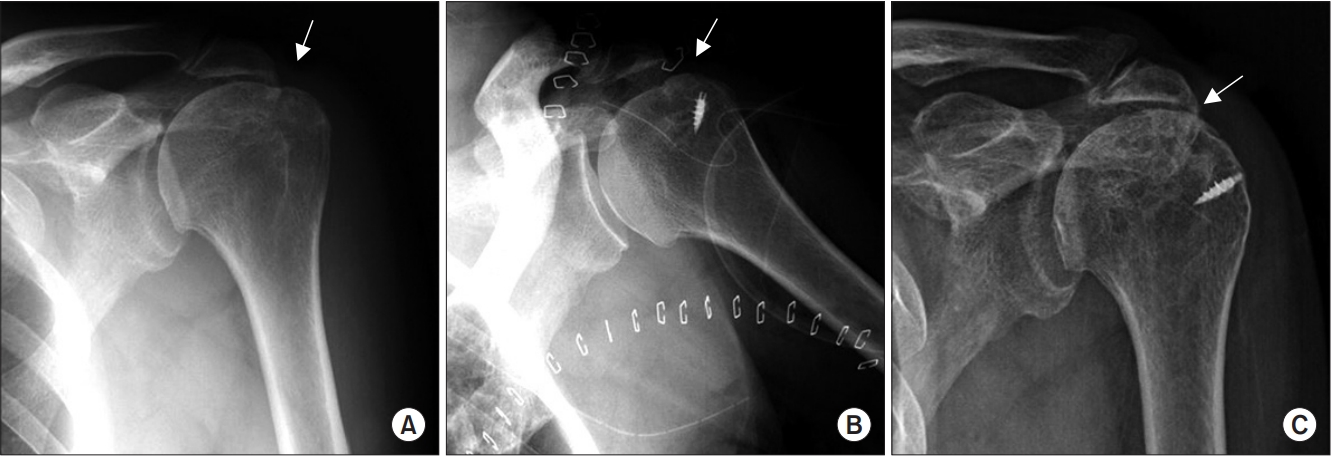
Comparison of preoperative and postoperative X-ray shows significant change in the mean distance of the acromiohumeral interval (p<0.05). Preoperative acromiohumeral interval (A, arrow) increases after lattisimus dorsi tendon transfer (B, arrow). At postoperative 12 years, the acromiohumeral interval (C, arrow) has decreased.
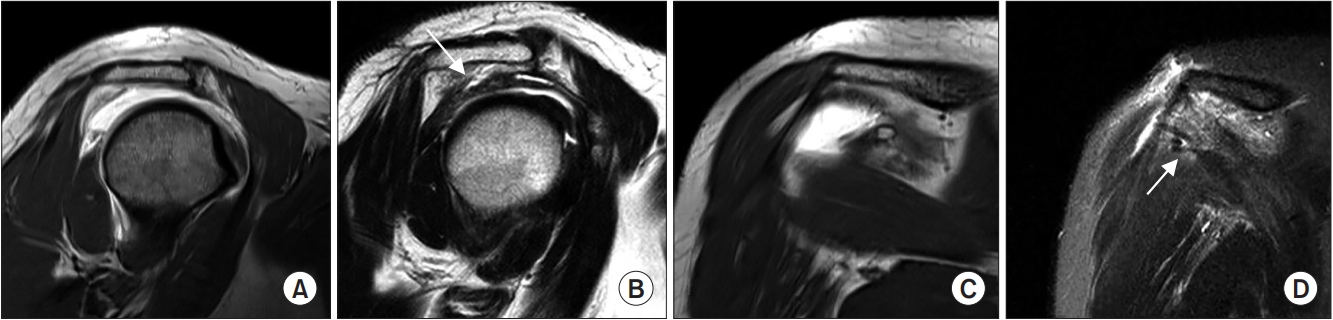
(A, C) Preoperative sagittal and coronal magnetic resonance imaging (MRI) revealed a complete torn cuff. (B, D) Postoperative follow-up sagittal and coronal MRI show transferred lattisimus dorsi tendon (arrow) to the tuberosity.
At the last follow-up, complications were observed in 5 patients (21.7%), including 3 tear and 2 infections; there was 1 case of deltoid detachment. Revision operation (repair) was performed in 2 patients with re-tear. Arthroscopic partial repair of the remnant cuff and debridement was performed. Both patients developed septic arthritis of the operated shoulder joint; 1 patient initially had deltoid detachment and got operated for the same reason. For 10 years after this surgery, the patient was able to work as a farmer, despite radiological progression of osteoarthritis on sequential follow-up X-rays. Delayed infection developed at postoperative 10 years, and PROSTALAC insertion was performed. The patient refused further revision surgery (Fig. 5). In another patient, arthroscopic debridement and irrigation was performed for early infection (2 weeks), which resulted in curing the infection.
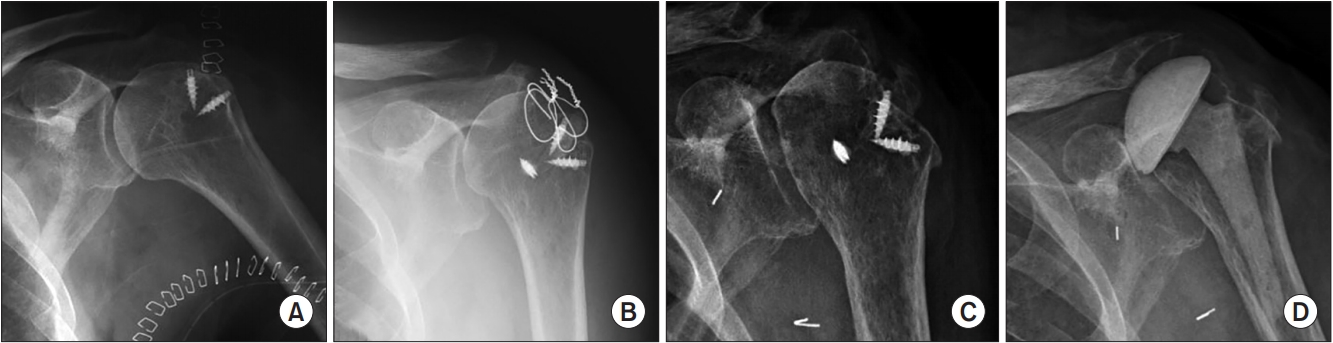
(A) After latissimus dorsi tendon transfer, at postoperative 10 years. (B, C) Complications of the latissimus dorsi tendon transfer are observed. Development of progressive osteoarthritis. (D) Insertion of PROSTALAC.
Discussion
The most important finding of the present study was that LD transfer for massive irreparable rotator cuff tears provides satisfactory clinical outcomes at mid-term follow-up periods. Complications such as tear, infection and mild degenerative osteoarthritis (stage 1, 2) of the shoulder joint are common at the midterm follow-up. However, our study showed significant increase in mild or moderate osteoarthritis (stage 1 or 2).
LD transfer is an anatomically & mechanically ideal method to restore active external rotation and to prevent further flexion impairment [18]. However, normal triceps and scapular muscles are prerequisites for this surgery. Also, the teres minor is important for the quality of comprehensive external rotation.
In a systemic review of 10 studies (mean age 58.7 years, and follow-up 45.5 months [24 to 126 months]), the mean adjusted constant score of 45.9 preoperatively improved to 73.2 postoperatively after LD transfer (p<0.001) [19]. Mean active forward elevation and external rotation improved from preoperative 101.9° and 16.8° to postoperative 137.4° and 26.7°, respectively (p<0.001). This review shows that LD transfer does not eliminate the potential for glenohumeral joint arthropathy, and the data presented demonstrates mean worsening of the osteoarthritis grade and acromiohumeral distance, as well as increasing superior migration of the humeral head in >50% of shoulders after the procedure. Also, this review reports that subscapularis muscle insufficiency, advanced teres minor muscle atrophy, and the need for revision surgery are correlated with poor functional outcomes.
Long-term pseudoparalysis is a contraindication of LD transfer, and age has no impact on the prognosis of elderly patients, except for elderly patients with generalized weakness. The upward migration of the humeral head could affect the clinical results, and Hamada classification 3 showed poorer clinical outcomes. Pre-existent degenerative arthritis could also progress rapidly after LD transfer.
LD transfer is effective in recovering active external rotation, but only at partial or varying degrees. Moreover, recovery is better in the early stages of an external rotation disorder or in the case of a damaged teres minor [18]. Recovery of abduction and external rotation remains controversial. There is also controversy about the ideal attachment site of the transferred LD. A supraspinatus insertion is normally favored for LD transfer since it provides maximal external rotation with minimal resistance to humeral abduction [20]. Considering the biomechanical aspect, there are assertions that the greater tuberosity is superior to other sites for improving range of motion of the transferred tendon, but, conversely, there is a claim that the additional tenodesis effect is obtained by fixation at the anterior aspect of greater and lesser tuberosity. More than half the active external rotation moment was restored by transferring LD to either supraspinatus or subscapularis insertion. Comparatively, only 20% of the external rotation moment was restored when the attachment site was at the teres minor insertion. When LD was transferred to the infraspinatus insertion, the external rotation moment was higher, as compared to the healthy state [18].
Gerber et al. [11] reported on long term results, with a minimum 10 years follow-up; their study indicates inferior results/outcomes in the subscapularis insufficiency and fatty infiltration of teres minor tendon. Also, superior functional results were associated with small postoperative critical shoulder angle.
Nove-Josserand et al. [21] operated 30 patients between 2001 and 2004, using Gerber’s method in 26 patients. The indications for surgery were difficult to repair supraspinatus and infraspinatus tendon rupture, and having higher than grade 2 fatty degeneration or with severe limitation of external rotation, regardless of age or fatty degeneration. The mean SSV was 68% ± 17%; the constant score improved from 50 ± 12 to 74 ± 9, and the adjusted constant score improved from 62 points to 91 points. External rotation improved by an average of 7°, whereas hornblower sign showed improvement in 6 patients but persisted in 9 patients. The number of patients unable to eat or drink decreased from 64.7% to 8.0%. Good improvement was observed in severe limitation of external rotation or teres minor tear, but there was no improvement in the muscle strength. The authors maintain that the patients have higher satisfaction due to alleviation of pain and improvements in simple daily life functions such as eating food and drinking. There remains a complexity in analyzing the movement mechanism of the transferred tendon (special exercise mechanism or tenodesis effect) and the cause of failure. There is no definitive answer to the position and fixation of the transferred tendon (anterior or posterior tuberosity), until now. However, the reason for poor results in many cases may be the failure of adequate fixation.
Electromyography studies have confirmed electrical stimulation of the transferred LD, but their effect in recovery of active external rotation is variable and controversial. The present results indicate that the transferred tendon works by compensating for impairment of the teres minor. The most appropriate indications for LD transfer could therefore include posterosuperior rotator cuff tear, difficult to repair, severe loss of external rotation, and active abduction with impaired teres minor function. However, failure to restore muscle weakness is an important complication of LD transfer.
Our study has several limitations. The most important limitation is the small number of patients. More long-term follow up evaluations with larger volume are required. Also, there is no comparative study with other methods such as partial repair, tendon augmentation or superior capsule reconstruction.
Conclusion
LD transfer provides satisfactory clinical outcomes at the midterm follow-up periods in massive irreparable rotator cuff tears. In the current study, LD transfer resulted in significant improvements in both function and pain relief. However, complications such as re-tear, infection and degenerative osteoarthritis of the shoulder joint were common during the mid-term follow-up.
Notes
Research Ethics
IRB approval: The Catholic University of Korea, Daejeon St. Mary’s Hospital (No. DC19RESI0034).
Conflict of interest
None.
Financial support
None.