INTRODUCTION
Intra-articular distal humerus fractures are uncommon injuries, with a reported incidence of 5.7 to 8.3 per 100,00 people per year [1,2]. These fractures are challenging to treat and often require surgical intervention. In younger patients with good bone quality and higher functional demands, the preferred surgical option is open reduction and internal fixation (ORIF). Studies have shown that the functional outcome after fixation of intra-articular fractures is directly related to the quality of reduction, especially the joint surface [3,4].
The recreation of three-dimensional (3D)-printed models of fractured bone from computed tomography (CT) data could be beneficial for preoperative planning of complex cases. To improve visualization of the fracture with conventional imaging modalities, 3D models allow a better sense of the fracture fragments and manipulation needed prior to the actual surgery. Such models also allow creation of patient-specific custom implants that better suit individual anatomy [5].
Despite these benefits, 3D printing is not routinely used in preoperative evaluation and surgical planning of distal humerus fractures. It is unclear if application of 3D printing will significantly improve functional outcomes. Hence, we conducted this systematic review and meta-analysis to answer the following questions: (1) Does the application of 3D-printed models of distal humerus fractures lead to quicker surgeries, with a reduction in need for fluoroscopy? (2) Do these surgeries result in less blood loss compared with conventional methods? (3) Is the complication rate lower for surgeries operated with 3D printing assistance, and do they have a better overall functional outcome?
We hypothesized that 3D printing would lead to quicker surgeries with less use of fluoroscopy and fewer complications, potentially improving final clinical outcomes. This research draws a detailed comparison of cases operated using 3D-printed models with those performed using conventional techniques to offer better evidence in favor or against this technology. To the best of our knowledge, there have been no previous systematic reviews on this topic.
METHODS
Because this is a systematic review article and we did not process individual patient data, ethics approval was not deemed necessary.
Protocol and Registration
This study was conducted based on an a priori protocol that was registered in MedRxiv.org as ID MEDRXIV/2022/269836 [6].
Search Methodology
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Fig. 1). We conducted a literature search in the electronic databases of Medline (PubMed), Embase, Ovid, and Scopus, on August 6, 2022. The detailed search strategy and the corresponding number of hits are shown in Table 1. Articles published from inception until the search date were included in this study. Duplicate articles and non-English studies were removed. Once eligible articles were finalized, a bibliography search was performed to identify additional studies.
Participants, Intervention, Control, and Outcome Framework for the Study
Participants: Adult patients with an intra-articular distal humerus fracture requiring surgery. Intervention: 3D printing-assisted ORIF. Control: conventional ORIF without the use of 3D printing.
Inclusion and Exclusion Criteria
The detailed inclusion and exclusion criteria are given in Table 2.
Data Extraction
Literature search results were screened by two authors (VB and SP) based on title and abstract. Inclusion and exclusion criteria were applied to select eligible articles. In cases of uncertainty regarding inclusion of any article, full texts were obtained and reviewed. Any conflict with respect to the inclusion or exclusion of a particular study between the two authors was resolved by mutual discussion with the other authors. The data from eligible studies were extracted into spreadsheets, including the name of the first author, study design, number of patients, mean age, mean operating time, blood loss, radiation exposure, complication rate, functional outcome, postoperative range of motion, and time to fracture union.
Assessment of Risk of Bias
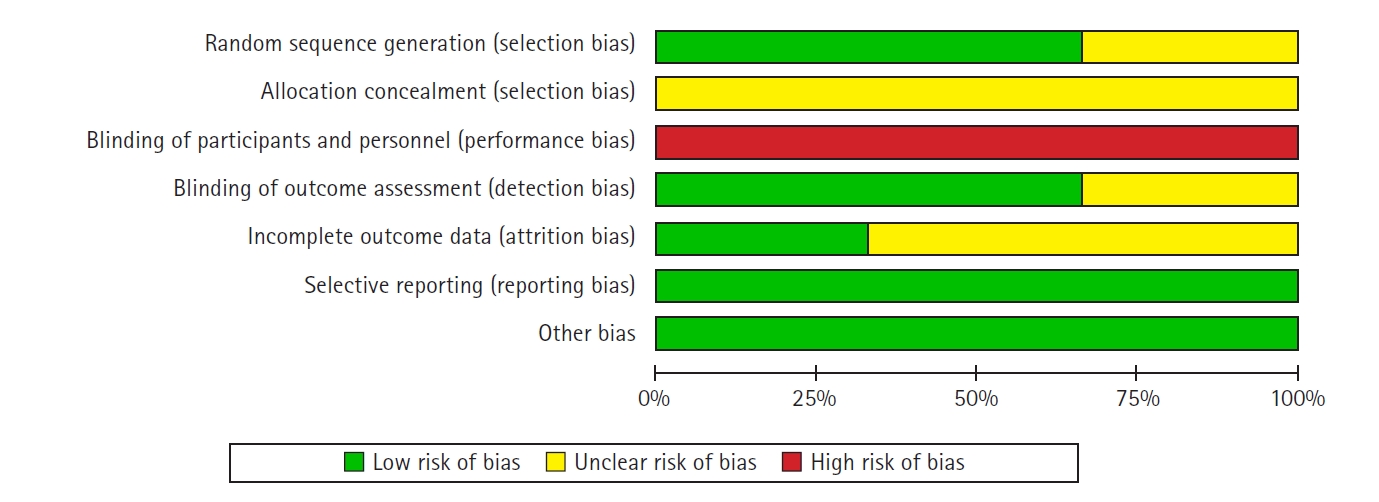
The Cochrane risk-of-bias tool for randomized controlled trials was used to evaluate risk of bias in the included studies by two authors separately (VK and SS) [7]. The tool included seven items on generation of random sequence, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and other biases.
Statistical Analysis
A meta-analysis was carried out comparing the outcomes of the group that underwent 3D-printing–assisted surgery with that of the conventional surgery group. Continuous variables were assessed with inverse variance weighted analysis, and the results are depicted using mean differences. Mantel-Haenszel odds ratio estimates were used for dichotomous variables. The I2 statistic was used to report heterogeneity in the articles. A random-effects model was chosen whenever I2 was greater than 50%, and in all other cases, a fixed-effect model was used. For analyses, 95% confidence intervals (CIs) were used, with a P-value ≤0.05 considered statistically significant. Meta-analysis was conducted using Review Manager (RevMan computer program ver. 5.4.1, The Nordic Cochrane Center, The Cochrane Collaboration, 2014).
RESULTS
Search Results
The literature search yielded a total of 6,389 results, and 6,377 studies were excluded after screening by title and abstract and removing duplicates. The full texts for the remaining 12 articles were obtained. Nine articles were further excluded because they were review articles (n=3), non-clinical studies (n=4), or conference abstracts (n=2). Finally, three studies were selected for the final analysis.
Study Characteristics
This meta-analysis included three randomized controlled trials with data on 144 patients with a mean age of 42.9 years. There were 87 males and 57 females. Sixty-nine cases were operated on with the help of 3D-printed models, and 75 patients underwent surgery without 3D printing assistance. Table 3 summarizes the characteristics of included studies [8-10]. AO/OTA type 13C (complete articular) fractures were included. All the studies used Mimics software (Materialise) to reconstruct the 3D models from CT data. The 3D printers used were SRP400B (Huasen 3D Printing Research), 3D Ortho (Waston Med Inc.), and 3D printer (Flashforge Ltd.).
Risk of Bias
The risk of bias assessment in the included studies resulted in some concerns (Fig. 2). The domain of "blinding of participants and personnel" had the highest risk of bias, with no studies following the practice. We conducted the meta-analysis despite this increased risk of bias because it is not practically feasible to blind the operating surgeon to the procedure.
Clinical Outcomes
Mean operating time
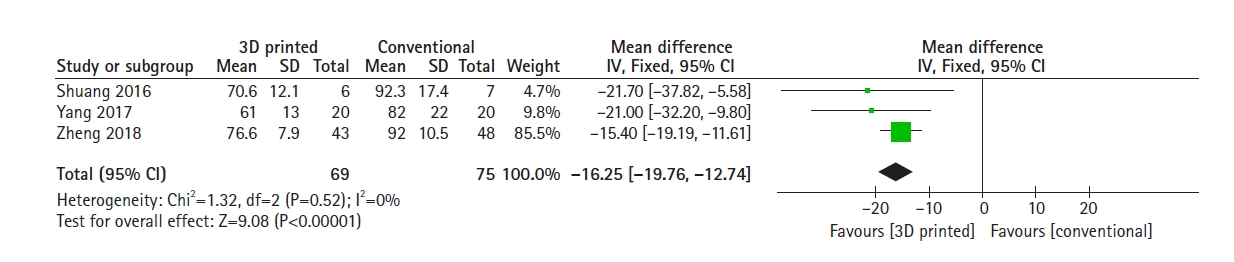
All included studies had data on mean surgical duration. The 3D-printed–assisted surgical group had significantly shorter mean operating times compared with the conventional group (mean difference, 16.25 minutes; 95% CI, 12.74–19.76 minutes; P<0.001) (Fig. 3).
Rate of complications
All studies included data on complication rates. There were six instances (8.7%) of complications occurring in the 69 cases performed with 3D printing assistance and 11 (14.7%) complications among the 75 patients that received conventional surgery (infections). The complications reported were wound infection and ulnar neuropathy. The 3D-printed group tended to have an overall lower complication rate; however, this was not statistically significant (odds ratio, 0.57; 95% CI, 0.21–1.58; P=0.28) (Fig. 5).
Rate of excellent and good outcomes
All studies assessed functional outcome using the Mayo elbow performance score. A score ≥90 points is classified as excellent, 79–89 points as good, 60–74 points as fair, and <60 points as poor outcome. The patients that were operated on with 3D printing assistance tended to have a more frequent good or excellent outcomes (odds ratio, 1.79; 95% CI, 0.78–4.10). However, this difference did not reach statistical significance (P=0.17) (Fig. 6).
DISCUSSION
Distal humerus fractures present distinct challenges for the treating surgeon owing to their complex anatomy, soft tissue injuries, and excessive load on the implants. Inadequate reduction of joint surface leads to inferior functional outcomes. Therefore, proper preoperative planning is crucial, and use of 3D-printed models could play an important role in managing these fractures.
Our systematic review revealed that application of 3D printing-assisted surgery produced significantly better outcomes than conventional methods in terms of quicker procedures with less intraoperative blood loss. Patients who underwent surgery with 3D printing also had a lower rate of perioperative complications and better overall functional outcomes than conventional surgery patients, but this difference was not statistically significance. Similar results have been reported in studies focusing on other intra-articular and complex injuries such as tibial plateau fractures, pilon fractures, pelvic-acetabular fractures, proximal humerus fractures, and revision total hip arthroplasty [11-16].
The group with 3D-printed models consistently demonstrated reduced surgical duration. Nevertheless, a more comprehensive assessment is necessary to determine the clinical significance of these time savings. Prolonged operating time is directly linked to the incidence of perioperative complications [17]. Although the difference in complication rate among the two the groups did not reach statistical significance, the significant reduction in surgical duration due to 3D printing-assisted surgery could potentially decrease the incidence of complications, especially infections. The significant decrease in blood loss with the help of this technique could also play a role in reducing postoperative anemia-related complications.
In the articles assessed in this review, 3D printing was primarily used for preoperative planning, wherein 3D-printed models are physical replicas that demonstrate the fracture's distinct morphology and allow the surgeon to carry out simulated reduction maneuvers. These models could be used to plan the ideal surgical approach and the direction of screws, for implant selection and positioning, and to determine the requirements for bone grafts. This technique could greatly help amateur surgeons in their surgical planning of multi-fragmentary articular fracture patterns (AO type C3).
Despite the various benefits, this technique does have some drawbacks. The added costs involved in preparing the 3D models are generally passed on to the patients, increasing their economic burden. According to Yang et al. [9], the cost of printing a 3D model was only U.S. $ 2–3; however, this does not account for the capital required to set up the printing facility, which requires expensive instruments likely beyond the budget of low-volume clinics. Complex 3D models require time for preparation and printing, limiting their application in emergency cases or open fractures. These limitations notwithstanding, because setting up a 3D printer is a one-time investment, and since this technique may be applied to other areas such as fractures of the proximal humerus, pelvis/acetabulum, and in arthroplasty cases, we recommend 3D printing facilities for centers that have sufficient capital and caseloads.
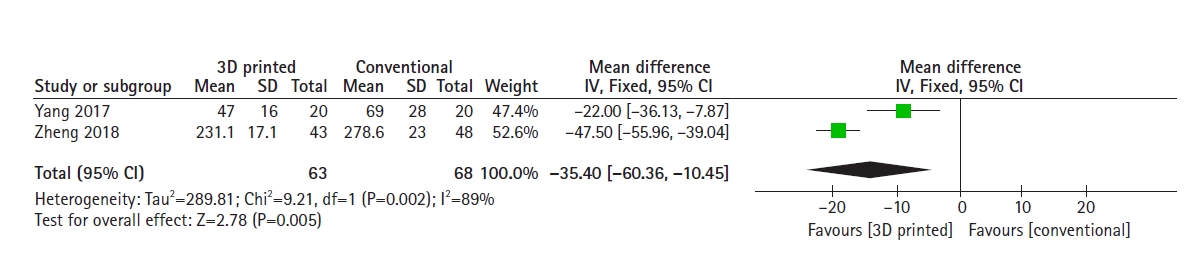
This meta-analysis also has a few limitations. Because a primary outcome was not defined, the potential for type-I and type-II errors is inflated. The included studies did not report a sufficiently long follow-up to account for long-term complications such as secondary osteoarthritis. The relatively small overall sample size could also explain why some results did not reach statistical significance. The lack of blinding of participants and personnel in most studies may have also led to bias. Yang et al. [9] and Zheng et al. [10] provided data on blood loss, but Shuang et al. [8] did not, which restricts the potential for a comprehensive pooled analysis. Due to the limited number of studies and their potentially diverse contexts, the findings may not be universally applicable.
Despite these limitations, there are several strengths to this review. To the best of our knowledge, this is the first meta-analysis evaluating the utility of 3D printing in the fixation of distal humerus fractures. We strictly followed a pre-defined study protocol. All the included studies were randomized controlled trials, giving rise to the best quality of synthesized evidence. There was uniformity in reporting the outcomes between all the studies.
CONCLUSIONS
Application of 3D printing assistance in distal humerus fractures—especially AO type 13C3, multi-fragmentary, complete articular fractures—leads to significantly shorter operating times and less blood loss, indirectly reducing the risk of infection. This technique could also potentially improve the reduction quality and postoperative functional outcomes, but more high-quality studies are required to generate sufficient evidence.