Reverse total shoulder replacement for patients with “weight-bearing” shoulders
Article information

Abstract
Background
Reverse total shoulder arthroplasty (rTSA) has gained popularity in recent years and is indicated for a wide variety of shoulder pathologies. However, use of rTSA in patients with “weight-bearing” shoulders that support wheelchair use or crutches has higher risk. The aim of this study was to assess the results of rTSA in such patients.
Methods
Between 2005 and 2014, 24 patients (30 shoulders) with weight-bearing shoulders were treated with rTSA at our unit. Patients had cuff arthropathy (n=21), rheumatoid arthritis (n=3), osteoarthritis (n=1), acute fracture (n=3), or fracture sequela (n=2). Postoperatively, patients were advised not to push themselves up and out of their wheelchair for 6 weeks. This study was performed in 2016, and 21 patients (27 shoulders) were available for a mean follow-up of 5.6 years (range, 2–10 years). The mean age at surgery was 78 years (range, 54–90 years).
Results
Constant-Murley score improved from 9.4 preoperatively to 59.8 at the final follow-up (P=0.001). Pain score improved from 2/15 to 13.8/15 (P=0.001). Patient satisfaction (Subjective Shoulder Value) improved from 0.6/10 to 8.7/10 (P=0.001). Significant improvement in mean range of motion from 46° to 130° of elevation, 14° to 35° of external rotation, and 29° to 78° internal rotation was recorded (P=0.001). Final mean Activities of Daily Living External and Internal Rotation was 32.4/36 (range, 16–36). Only three patients showed Sirveaux-Nerot grade-1 (10%) glenoid notching and three grade 2 (10%).
Conclusions
rTSA can be used for treatment of patients with weight-bearing shoulders. Such patients reported pain free movement, resumed daily activities, and high satisfaction rates.
Level of evidence
IV.
INTRODUCTION
Reverse total shoulder arthroplasty (rTSA) has gained popularity in recent years. Currently, it is indicated for a wide variety of shoulder pathologies including cuff tear arthropathy, irreparable rotator cuff tear, proximal humeral fracture, fracture sequela, and revision of failed arthroplasty. The shoulder is a common site of upper extremity pain in patients with ‘weight-bearing’ shoulders [1], those that are using wheelchairs and crutches for ambulation [2]. Shoulder pain is reported in 38%–67% of patients using wheelchairs for mobility [2]. Often, the pain gradually becomes worse [3,4] and significantly affects the patient’s quality of life. Problems arise from patients’ use of their shoulders to mobilize and transfer their body weight [5] when relying on crutches or wheelchairs [2].
Constant use of the shoulders for all daily activities causes a higher incidence of shoulder problems among this patient group. The situation is worsened because resting is not often feasible given that the upper limbs are needed for propulsion and locomotion. Despite the high prevalence of shoulder pathology in patients with weight-bearing shoulders, there is little discussion in the literature regarding surgical treatment and outcomes, especially of rTSA [6-11].
Our unit is a referral center for shoulder conditions, and all our arthroplasty patients are prospectively entered into a dedicated database. We identified 24 patients (30 shoulders) with weight-bearing shoulders that were treated with rTSA for various pathologies over a period of 10 years. The aim of this study is to assess the clinical and radiographic results of rTSA in these patients with weight-bearing shoulders.
METHODS
Institutional Review and Audit Board of Royal Berkshire NHS Foundation Trust approved this study (no. N3114). Informed consent for the study was obtained from the patients, and approval for publication was obtained from the patient whose photos are used.
Patients and Characteristics
Between 2005 and 2014, 24 patients (18 female, 6 male) using mobility aids were treated at our center with rTSA for pain and severe limitation of function. Six female patients had bilateral shoulder arthroplasty. In total, 30 shoulders underwent operation, 21 (70%) for cuff arthropathy, 3 (10%) for rheumatoid arthritis, 1 (3.3%) for osteoarthritis, 3 (10%) for fracture, and 2 (6.7%) for fracture sequela. All patients had mobility problems: 19 used a wheelchair and 5 used crutches to ambulate. All patients were obligatory upper-extremity ambulators. Demographic data are detailed in Table 1, including the interval from onset of symptoms to rTSA, the number and type of prior procedures, the diagnosis requiring crutches/wheelchair, the duration of the weight-bearing status, hand dominance in relation to the rTSA, and the condition of the other shoulder at the time of surgery.
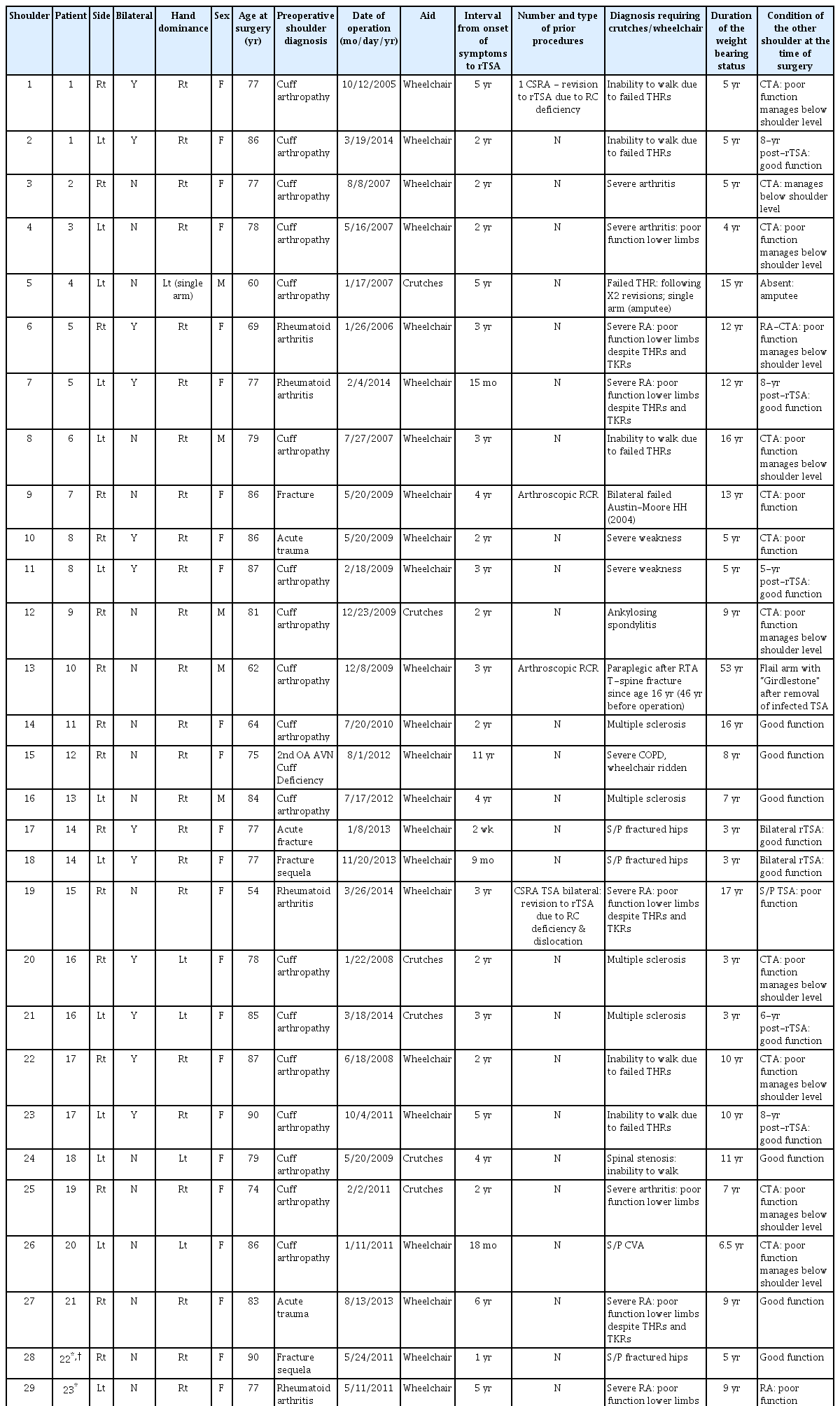
Patient demographics
Surgical Procedures
All operations were performed though the antero-superior Neviaser-MacKenzie approach. The deltoid was detached from the anterior acromion with an osteo-periosteal flap and restored to the acromion with the “double row” fixation technique at the end. Remnants of the subscapularis and teres minor were reattached to the humerus with sutures (Ethibond 5.0) whenever possible. When treating acute fractures, the tuberosities were fixed to the humerus shaft using a suture fixation technique (Ethibond 5.0). In all cases, the implant used was cementless with a dialable-sloped liner (Verso, Innovative Design Orthopaedics). The glenoid was inserted with 10º–15º of inferior tilt and the humeral component with 30º of retroversion. A stemless implant was favored when possible, but both were allowed based on circumstances. For cuff arthropathy, rheumatoid arthritis, and osteoarthritis, a stemless humerus shell was inserted. When treating acute fractures and fracture non-union, use of a stemmed implant depended on the amount of bone loss and was assessed intraoperatively. If the stemless implant was stable or could be made stable with bone impaction grafting, then such an implant was used; if not, a stemmed implant was used to provide fixation. In our series, one stemmed and one stemless implant were used for fracture sequelae and three stemmed implants were used for acute proximal humerus fractures. Overall, 26 short metaphyseal stemless and four stemmed implants were used. The glenoid baseplate had a tapered central screw with two additional anti-rotation screws, positioned at superior and inferior locations.
Rehabilitation
Rehabilitation was initiated immediately postoperatively with shoulder pendulum and passive range of movement exercises followed by a deltoid rehabilitation regime [12]. A sling was used for 3 weeks, and patients were advised to neither push themselves out of their chair, transfer themselves from their car, nor to use crutches for 6 weeks. Postoperative rehabilitation was the same as in non-weight-bearing patients, but these patients had to avoid transfers and had to be closely supported by family members or reside in a convalescent institution for the first 6 weeks postoperatively.
Data for all patients were prospectively collected and stored in a dedicated database (MS Access). Demographic data, operation details, and preoperative and postoperative assessments were recorded. Clinical and radiographic assessment was performed postoperatively at 3 and 6 weeks, 3, 6, and 12 months; and then yearly thereafter. Outcome measures were visual analog pain score [13], Constant-Murley Score (CMS) [14], and Subjective Shoulder Value (SSV) [15]/Single Assessment Numeric Evaluation (SANE) [16]. Video recording of the patients range of motion and function was recorded preoperatively and in every follow-up visit for all the patients.
Additionally, the quantification of Activities of Daily Living (ADL) that require active external rotation (ER) and internal rotation (IR; ADLEIR) score, was recorded using a dedicated template (Fig. 1). Boileau et al. [17] initially introduced the ADLER score to evaluate more objectively the potential effect of active ER on ADLs (quantification of ADL that require active ER, or ADLER). The score was designed with a given number of points according to the severity of the potential handicap: unable (0 points), very difficult (1 points), somewhat difficult (2 points), or not difficult at all (3 points). All activities should be performed without flexing the neck or bending the trunk and without first abducting the elbow (i.e., without a “horn blower sign”). A maximum score of 30 points indicated the patient was able to easily perform all 10 tasks of the ADLER score. The ADLER score was introduced and validated by Boileau et al. [17,18] and has been used in several publications [17-19].

The Activities of Daily Living External and Internal Rotation (ADLEIR) score form.
We added two further important ADLs that require active IR with the same grading system. The ADLEIR score is the sum of the quality and ease of the patient to perform each of these activities. A maximum score of 36 points indicates that the patient was able to easily perform all 12 tasks of the ADLEIR score (Fig. 1).
Radiographic Assessment
Radiographic analysis was performed using a true anteroposterior and axillary views of the shoulder.
Video Recording
Range of motion (ROM) and function were recorded on video preoperatively and at all clinical follow-up visits for all patients.
Statistical Methods
Data were collected prospectively and recorded using a dedicated MS Access database. Improvement, or gain, in both functionality (CMS) and SSV [14] or SANE [15] were calculated for each case by comparing the latest observed postoperative value to the corresponding preoperative value, and the significance of the difference was tested using the paired t-test. Statistical analyses were performed using SAS (Release 8.2; SAS Institute Inc).
RESULTS
This study was performed in 2016. Two patients died from unrelated causes and one patient that lives far from the unit refused to come for clinic appointment claiming that there was no reason since her shoulder caused no problems in life and daily activities. For the remaining 21 patients (27 shoulders), the mean follow-up was 5.6 years (range, 2–10 years), and the median age at surgery was 78 years (range, 54–90). Mean CMS improved from 9.4 points (range, 2–26) preoperatively to 59.8 points (range, 29–80) at final follow-up (P=0.001). Pain (measured as a part of the Constant score) improved significantly from a mean 2/15 (range, 0–8) preoperatively to 13.8/15 (range, 9–15) (P=0.001). Patient satisfaction (SSV [15]/SANE [16]) increased from 0.6/10 to 8.7/10 (P=0.001) at final follow-up (Table 2, Figs. 2 and 3).

Preoperative and at final follow-up of pain, Subjective Shoulder Value, Constant-Murley score, and ADLEIR scores

Preoperative and final follow-up values for Constant-Murley score, pain score, Subjective Shoulder Value (SSV), elevation, and external and internal rotation.

(A) Sixty-two-year-old paraplegic patient with bilateral rotator cuff arthropathy. Left shoulder after infected total shoulder arthroplasty (TSA) with resection arthroplasty. Preoperative range of motion of the right shoulder with rotator-cuff arthropathy. (B) The same patient 4 years after reverse TSA. a: elevation, b: abduction, c: external rotation, d: anteroposterior X-ray.
Significant improvement in mean ROM in all directions was recorded. Elevation improved from a mean of 46º (range, 0º–120º) to 130º (range, 30º–180º) (P=0.001). ER increased from 14º (range, 0º–80º) to 35º (range, 30º–80º) (P=0.001). IR improved from 29º (range, 0º–90º) to 78º (range, 20º–90º) (P=0.001) (Tables 2 and 3, Figs. 2 and 3). Final mean ADLEIR score was 32.4/36, indicating that most patients were able to perform ADLs (Table 2). Table 4 shows the individual scores for each of the ADLs in the ADLEIR score for each shoulder in the study. Sequential plain radiologic follow-up revealed no instability, no subsidence, no stress shielding, and no implant loosening. There were three Sirveaux-Nerot [20] grade 1 (10%) and three grade 2 (10%) glenoid notchings.

Preoperative and at final follow-up ROM

Detailed results of each individual activity of the ADLEIR score for each patient’s shoulder
Complications
No dislocation or humeral or glenoid loosening was encountered in our series. Two patients experienced reduction in shoulder function and greater than average pain due to injury from a fall. One sustained a proximal humerus fracture and the other suffered a scapular spine fracture. Both were treated conservatively, but range of movement and patient satisfaction decreased after the fall.
DISCUSSION
Shoulder pain is common among patients with weight-bearing shoulders, reported in 39.8% of chronic spinal cord injury patients using mobility aids [2]. Despite the high prevalence of shoulder pain and shoulder pathologies among patients with weight-bearing shoulders, there are very few evaluations of their surgical treatment. Jung et al. [21] reports successful repair of rotator cuff tears in 15 patients, and Garreau De Loubresse et al. [6] showed similar results from anatomic TSA in five patients with osteoarthritis. Nevertheless, Kemp et al. [11]recently reported a higher complication rate in 12 patients undergoing rTSA. The fact that this population of patients rely on their shoulders for mobilization makes both surgeons and patients reluctant to engage in surgery, and the small numbers of reports in the literature makes this discussion even more difficult. For the same reason rehabilitation and outcome can be lengthy and unpredictable.
ADL have been shown in vitro to load the glenohumeral joint (GHJ) with a weight greater than a person’s body weight [22]. Forces loading the GHJ of patients using wheelchairs or crutches are not significantly higher than those of ADL [23,24], although lifting oneself from a wheelchair can involve si gnificantly higher load of up to 188% of body weight [23]. This may explain why patients using crutches and motorized wheelchairs experience more frequent shoulder pain than manual wheelchair users, even though the difference is not significant [2]. Other research explained that patients dependent on crutches or a wheelchair may be more prone to shoulder injury due to repetitive movements involved in ambulation rather than the actual load on the GHJ during mobilization [23,24]. All patients in our present study were obligatory users of a wheelchair or crutches (obligatory upper limb ambulators). Regardless of the reason for their reliance on these aids, they all had to transfer their weight using their upper limbs, exerting their body weight through the shoulders.
Patients with weight-bearing shoulders have different joint biomechanics. Altered kinematics and frequency of movement may lead to higher risk of failure following rTSA. Studies on shoulder kinematics [7-9] of wheelchair users have identified changes in scapulothoracic and glenohumeral movement and orientation. Propulsion, transfer, and weight relief lifts involve scapulothoracic upward rotation, along with and internal scapular rotation and anterior lift. Simultaneously, large degrees of humeral transverse translation and ER of the GHJ occur. Finally, the shoulder joint is loaded in the superior direction more heavily in weight relief lifts and transfers, but also during propulsion. This results in superior translation of the humeral head toward the subacromial space [5,25].
These changes in biomechanics mean that rTSA in weight-bearing shoulders is subjected to altered forces. Of great importance is the scapulothoracic upward rotation. It has been shown that 15º of inferior tilt provides uniform loading forces along the baseplate [10]; upward scapular rotation compromises this balance. Increased torque and shear forces on the glenoid component caused both by superior loading of the GHJ and scapulothoracic upward rotation can cause loosening of the glenoid component [26], and increased external glenohumeral rotation is common among weight-bearing shoulders. In contrast, ER deficit is common after rTSA [27] and could lead to significantly increased loads across the implant in weight-bearing shoulders. Implants that provide increased ER and the ones with lateralized offset [27] may be better for this reason. However, lateralized implants may have higher risk of glenoid loosening [28] that increases with superior translation of the humeral head toward the subacromial space and scapulothoracic upward rotation.
Although propelling a wheelchair is different from using crutches for ambulation, biomechanically, both rely on weight-bearing shoulders for transfers and ambulation. Both groups have theoretical increased risks for dislocation, wear, and failure. Reverse shoulder arthroplasty was initially designed for rotator-cuff arthropathy [29] but has since been successfully extended for use with all types of arthropathy and osteoarthritis of the GHJ [30], proximal humerus fractures [31], and fracture sequelae [32].
Kemp et al. [11] recently published a study on 16 of 19 shoulders in wheelchair-dependent patients that underwent rTSA. Only 12 shoulders in 10 patients were available for a mean follow-up of 40 months (range, 22–66 months). The implant systems used were Equinoxe (Exactech Inc.) in eight patients and Encore RSP (Don Joy) in 4. Three patients experienced implant failure shortly after surgery (failure rate of 15.8% of eligible cases). They also reported major complication in of the 16 shoulders (25% complication rate) [11], a much higher complication rate than reported for patients in the general population undergoing rTSA with the Grammont prosthesis (20.7%) [33,34].
The early complications in Kemp et al.'s study [11] were reverse baseplate failure (baseplate loosening and dislodgement 6 weeks postoperatively) and dislocation (2 dislocations occurred approximately 3 months after surgery. One shoulder underwent a closed reduction that subsequently redislocated and was not reduced again, and the other shoulder was never reduced). A late complication, in Kemp et al.'s study [32], was periprosthetic humeral fracture due to loosening from infection. In Kemp study [11], not all patients were satisfied: 2 felt they were worse postoperatively; active elevation was 112°, and active ER was 29°; the glenoid notching rate was 42%.
Our relatively large series included 24 patients (30 shoulders), of whom 21 (27 shoulders) were followed for up to 10 years (mean follow-up, 67 months; range, 24–120 months). We found significant improvement in ROM, pain, patient satisfaction, and overall CMS. Active elevation was 130°, active ER was 35°, and active IR was 78°. The ADLEIR score was 32.4/36, indicating that most patients were able to perform ADL. Twenty-four of the shoulders could achieve active IR with their hand behind their back above the sacroiliac joint. Patient satisfaction was high at 8.7/10.
The design of the glenoid baseplate used in our series involves a central tapered screw that provides the main glenoid fixation. Hopkins and Hansen [35] compared six inverse-anatomy glenoid implants for ability to achieve primary stability through minimization of interface micromotion. The central tapered screw design baseplate (Verso) was most stable, with peak micromotion of 48 μm, lower than the other implants in the study. When comparing the baseplate complications and failures between the series, it is possible that different baseplate fixations may play a role.
Previous studies agree that mobility and upper limb function are closely linked in this group of patients, and indications for surgery should be comparable to those of the general population [6,21]. We had a similar experience and concluded that rTSA selection should be based on the diagnosis of the shoulder condition irrespective of the weight-bearing status. The main indication and most of our cases were cuff arthropathy (21 shoulders, 70%) or rheumatoid arthritis (3 shoulders, 10%). Osteoarthritis with deficient cuff (1 shoulder, 3.4%), complex fracture (3 shoulders, 10%), and fracture sequela (2 shoulders, 6.7%) were the other conditions treated.
Comparing the results of this study with results from rTSA with the same implant in the general (non-weight-bearing shoulder) population [19,36], we find similar outcomes relating to CMS (59 points in the general population, 59.8 in this study), ROM improvement, and SSV. ROM improvement was 129° active elevation in the general population compared with 130° in this study, active ER was 51° in the general population compared with 35° in this study, and active IR in the general population was 65° compared with 78° in this study. It seems that, among patients with weight-bearing shoulders, IR improves slightly more than ER. SSV was 8.5/10 in the general population compared with 8.7/10 in this study. The reason for better active IR in this group of patients is unknown. Possible explanation is that the wheelchair-bound patients need good IR to propel the wheelchair.
Postoperative rehabilitation in patients with weight-bearing shoulders is the same as for the general population. Pendulum, elbow, and wrist range of movement exercises start on the first postoperative day. Patients wear a sling for 3 weeks and are instructed to avoid pushing themselves out of their chair and to not use the arm to propel their wheelchair for 6 weeks [23]. For the same rehabilitation period, the use of crutches is restricted [24]. As these restrictions can cause significant reduction in mobility and restrict independence for this patient population, they should always be discussed with the patient prior to surgery during the consent process.
Limitations of our study are that our mid-term results were determined at a mean of 5.6 years post-surgery, and that it reports the experience of one center and one type of implant.
CONCLUSIONS
Reverse TSA can be used successfully and safely to treat patients with weight-bearing shoulders using a wheelchair. Patients report pain-free movement, resumption of daily activities, and high satisfaction rates. Indications and postoperative rehabilitation are the same as for all other patients. The first 6 weeks after surgery may involve significant reduction in mobility and independence of patients because of restrictions on using crutches and pushing themselves out of their wheelchair or transferring themselves. Patients should be aware and prepare for this accordingly.
Notes
Author contributions
Conceptualization: OL. Data curation: OL, GA, PC, OT. Formal analysis: OL, GA, PC, OT. Investigation: OL, GA, PC, OT. Methodology: OL, GA, OT. Project administration: OL, GA, PC. Resources: OL. Supervision: OL, PC. Validation: OL, GA, PC, OT. Visualization: OL, GA. Writing – original draft: OL, GA, PC. Writing – review & editing: OL, PC, OL.
Conflict of interest
None.
Funding
None.
Data availability
Contact the corresponding author for data availability.
Acknowledgments
None.