INTRODUCTION
Early accounts of the challenges surrounding gunshot wounds (GSWs) to the elbow date back to the Great War when Lieutenant-Colonel Mansell Moullin at London General Hospital described complications such as “acute septic inflammation;” eventual ankylosis; and ultimately, “deplorable” outcomes [1]. To this day, ballistic fractures near the elbow present a management dilemma for orthopedic surgeons. The challenges are often amplified by the soft tissue density of the elbow and associated risk of concomitant neurovascular injury. Nerve injuries near the elbow occur more frequently with fractures than with any other kind of trauma [2]. The kinetic energy dissipated by a ballistic missile traversing the soft tissue may result in a spectrum of nerve injuries from transient neuropraxia to complete neurotmesis. Penetrating trauma to the upper extremity may also result in vascular injury requiring repair [3]. In rare instances, isolated penetrating trauma to the upper extremity may result in initiation of a massive transfusion protocol and even death [4].
Traditionally, ballistic fractures in the extremities have been managed with prophylactic antibiotics, early debridement, and definitive stabilization with internal fixation. Recently, there has been a trend toward early definitive fixation, primary bone grafting, and more limited use of prophylactic antibiotics [5]. However, literature on the subject is sparse; optimal management strategies and reconstructive techniques remain unknown. Treatment options for penetrating upper extremity trauma and associated juxta-articular fracture include external fixators (both uniplanar and circular) [6-8], open reduction and internal fixation (ORIF) [9], total elbow arthroplasty [10], and amputation [11]. The use of polymethylmethacrylate, primary bone grafting, the induced membrane technique, or vascularized bone transfer may be necessary in cases of significant bone loss; however, there is no consensus in the literature regarding the timing and choice of bone-filling techniques.
This uncertainty surrounding treatment of these complex injuries warrants further investigation to optimize care for these patients. The purpose of this investigation was to review our level I trauma center experience with gunshot fractures near the elbow to identify common fracture patterns, characterize associated soft tissue and neurovascular injuries, and determine the effectiveness of our current treatment strategies.
METHODS
Approval from the Institutional Review Board of Baylor College of Medicine was obtained, and informed consent was not required due to the retrospective nature of the study. A retrospective review was performed to identify all patients who presented to a single urban level I trauma center from 2014 to 2018 with a periarticular gunshot fracture near the elbow. Demographic data, fracture pattern, and treatment type and outcomes were analyzed. Operative interventions, time to surgery, and antibiotic usage were recorded. Ballistic missile velocity was estimated by clinical history and radiographic fracture pattern. Low velocity was defined as less than 2,000 feet/sec and high velocity as greater than or equal to 2,000 feet/sec [12]. Fractures were classified using the AO classification system. Open fractures were classified according to the Gustilo-Anderson grading system [13]. Follow-up information was gathered if patients presented to the clinic after surgery.
RESULTS
Ninety-six periarticular fractures near the elbow presented to our level I trauma center during the 4-year collection period. Of these, 24 patients were identified with GSW-associated fractures. Demographic data are illustrated in Table 1. The average patient age was 38.3 years. Fourteen of the GSWs were considered low energy and 10 high energy. The location of fractures sustained are summarized in Table 2. Seven patients sustained isolated distal humerus fracture, 10 sustained isolated proximal ulna or proximal radius fracture, and seven had combined fracture pattern. Fractures are listed according to AO classification in Table 3.
Only five subjects (21%) sustained isolated GSWs to the elbow. The majority (79%) presented with multiple GSWs involving the chest, abdomen, spine, or additional extremity. Seven patients (30%) required emergent exploratory laparotomy upon arrival. Eleven patients (46%) were admitted directly to the surgical intensive care unit; the rest were admitted to lower-level nursing units.
Treatment Protocol
At our institution, initial efforts are directed toward the fundamental principles of Advanced Trauma Life Support protocols, "the ABCs.” After an initial primary survey in the emergency department, each patient presenting with a GSW to the elbow was evaluated by the orthopedic trauma team. Intravenous antibiotics were administered upon diagnosis, open wounds were irrigated at the bedside, and fractures were splinted in preparation for operative intervention. All patients received prophylactic antibiotics consisting of intravenous vancomycin and cefepime for 24 hours. This institutional protocol is based on local antibiotic susceptibilities and discussion with the Department of Infectious Disease.
All patients underwent urgent formal surgical debridement in the operating room. Definitive stabilization was achieved with internal fixation at the time of initial debridement unless there was associated vascular injury or soft tissue damage that precluded stable soft tissue coverage. Antibiotic-impregnated polymethylmethacrylate was used for bone gaps or articular defects. If the limb was dysvascular, vascular repair was performed prior to orthopedic intervention. If preoperative nerve palsy was present, the nerve was explored at the time of surgery.
The mean time to surgery was just over 72 hours but ranged from 5 hours to 10 days. In all cases, the limiting factor to surgical clearance was the presence of non-orthopedic injury and inadequate resuscitation. ORIF was performed at the time of initial debridement in 22 of 24 patients. One patient required debridement, antibiotic bead placement, and temporary elbow-spanning external fixation prior to ORIF due to contamination from the shotgun injury and a soft tissue defect that later underwent split thickness skin grafting. This was the only case of staged ORIF. One patient with a grade IIIC open proximal radius fracture developed a deep infection requiring multiple debridements. The presence of infection, combined with open fasciotomy wounds over the intended surgical approach, precluded ORIF of the underlying proximal radius fracture and repair of the associated posterior interosseous nerve (PIN) transection. The remaining 22 cases underwent early definitive ORIF at the time of initial debridement. Three patients with high-energy fracture patterns sustained bone loss necessitating fracture gap filling with antibiotic-laden polymethylmethacrylate.
Neurovascular Injuries
Two patients had concomitant arterial injury requiring repair. In both patients, brachial artery repair was performed emergently by the vascular surgery team prior to orthopedic intervention. Eleven patients (46%) had a nerve palsy affecting the ulnar, median, and/or radial nerve at the time of initial evaluation. Ten of the 11 patients underwent nerve exploration at the time of internal fixation, and all but two had a nerve contusion. The remaining two patients had nerve transections of the PIN in the context of isolated proximal radius fracture. Nerve reconstruction was not performed due to ongoing infection in one case. In the second, the location of the neurotmesis was at the branching point of the PIN into the extensor musculature, which combined with a large zone of injury, precluded nerve reconstruction. Both patients were treated with delayed tendon transfers.
Soft Tissue Injury
Eight patients sustained grade IIIA and two sustained grade IIIC open fractures. One patient required debridement, antibiotic bead placement, and temporary elbow-spanning external fixation prior to ORIF due to contamination from a shotgun injury and a soft tissue defect that later underwent split thickness skin grafting. No patient required free or rotational flap coverage.
Fixation Strategies
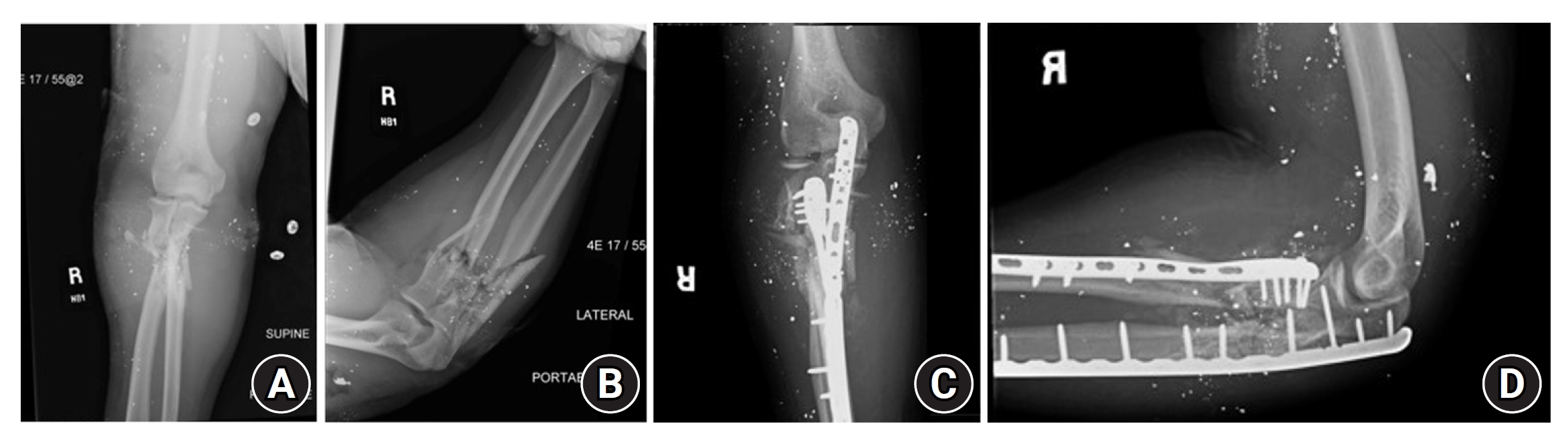
Standard fixation strategies included dual column plating for distal humerus fractures and periarticular locking plate fixation of proximal ulna and proximal radius fractures. Fracture comminution and meta-diaphyseal extension were frequently observed in this cohort, and alternate fixation strategies were needed in several cases. Three patients with high-energy fracture patterns sustained bone loss that necessitated fracture gap filling with antibiotic-laden polymethylmethacrylate. Fractures of the proximal ulna frequently required supplemental fixation, typically provided by suture augmentation of the triceps insertion. In one case (Fig. 1), the olecranon was deemed unreconstructable, and hybrid plate and screw fixation of the coronoid and suture fixation of the olecranon were required. Fractures of the proximal radius proved particularly challenging as fracture comminution typically extended beyond the span of most proximal radius specific plates. In such cases, a reversed distal fibular locking plate was employed, allowing fixation spanning from the radial neck into the diaphysis.
Ten fractures (42%) involved the distal humerus: five were extra-articular (AO type A), three were partial articular (AO type B), and two were complete articular (AO type C). Four of the extra-articular fractures were fixed with a 3.5-mm distal humerus locking compression plate (LCP), and one distal fracture was fixed with a 90–90 construct using 3.5/2.7 mm LCP medial and posterolateral distal humerus plates. One of the three partial articular fractures required an olecranon osteotomy, and the other two had concurrent olecranon fractures that provided adequate visualization of the articular surface. Two of the partial articular fractures were fixed with both lag screws and a neutralization plate (distal humerus 3.5/2.7 mm LCP), while one was fixed with independent lag screws. Of the two type C distal humerus fractures, one was associated with an olecranon fracture that provided adequate visualization of the articular surface. The other required an olecranon osteotomy. Both were fixed with 90–90 constructs using 3.5/2.7 mm, variable-angle LCP medial and posterolateral distal humerus plates (Fig. 2).
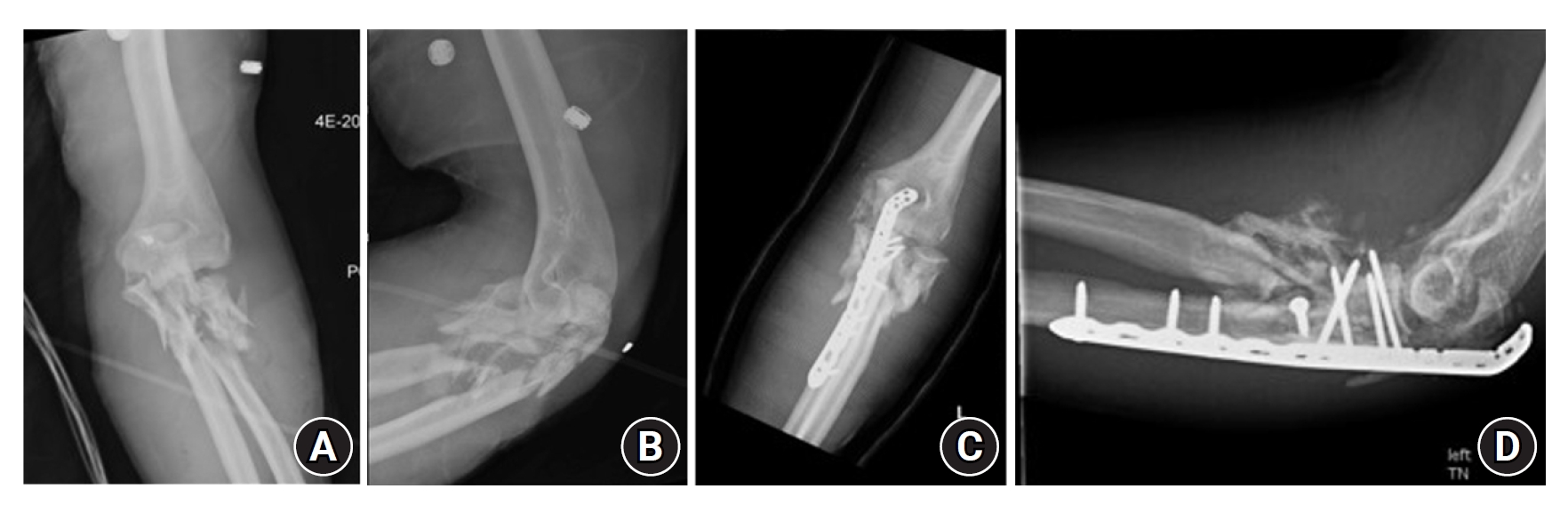
There were eight proximal radius fractures in the study: four were isolated and four were combined proximal radius and proximal ulna fractures. Of the four isolated proximal radius fractures, one associated with a grade IIIC open injury developed a deep infection and did not undergo implantation of hardware. The remaining three underwent ORIF. One of the reconstructive challenges unique to the proximal radius fracture cohort was the absence of adequate “real estate” for fixation in the proximal fracture segment. We devised a simple solution to this issue using a distal fibula LCP (3.5/2.7 mm LCP) to capture the proximal fracture fragment (Fig. 3). There have been no complications related to the use of this plate. Of the four patients with proximal ulna fractures, one non-displaced radial head fracture was managed nonoperatively, and one patient with proximal radius shaft fracture left the hospital prior to completing staged fixation of the radius. Of the remaining two patients, one underwent ORIF with a distal fibula locking plate, and one radial neck fracture was deemed unreconstructable due to severe comminution (Fig. 1).
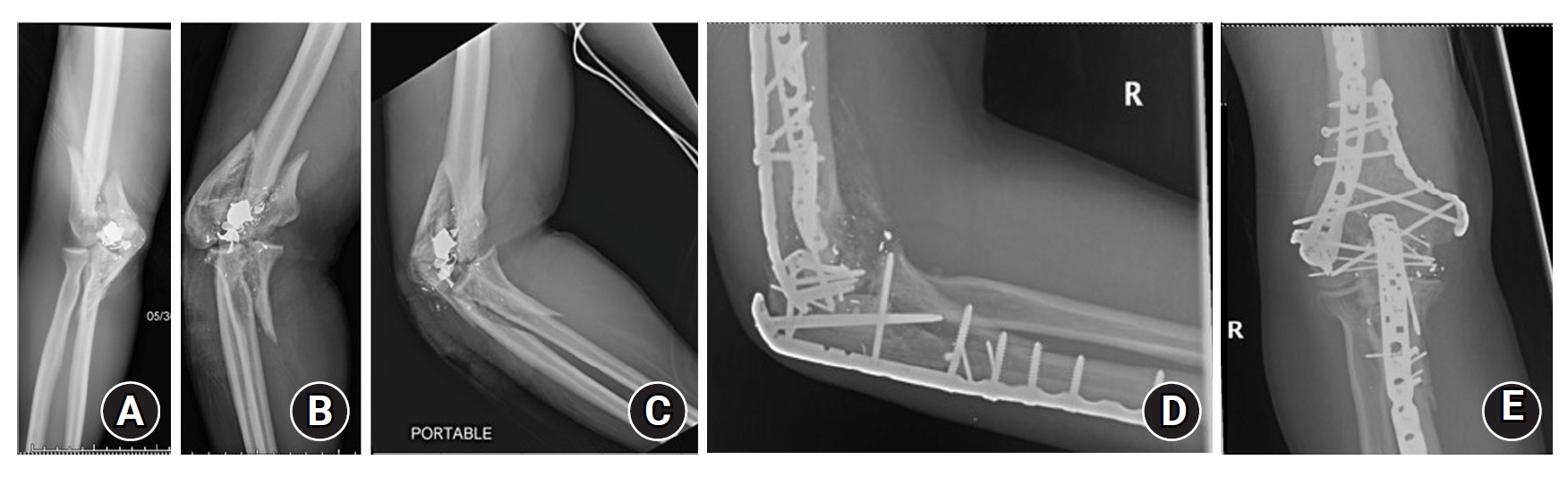
The third and final fracture cohort involves the proximal ulna. Thirteen patients sustained proximal ulna fractures, either independently (n=6) or in combination (n=7). All proximal ulna fractures were fixed using proximal ulna variable-angle LCPs. One complication was observed in this fracture cohort. At the 6-week follow-up visit, one patient who underwent ORIF of an isolated proximal ulna fracture displayed fracture displacement requiring revision ORIF (Fig. 4).
Complications
One patient developed a deep infection after a grade IIIC open proximal radius fracture requiring brachial artery repair and prophylactic forearm fasciotomy. Purulence extending from the fasciotomy to the open fracture was managed with application of antibiotic beads and multiple debridements. There were no other cases of postoperative infection following ORIF. One patient required revision ORIF due to loss of fixation of an olecranon fracture (Fig. 4). One patient with a deep infection went on to develop atrophic nonunion of a grade IIIC proximal radius fracture (Fig. 5). Six patients were followed-up long enough to determine bony union. Average follow-up was 12 weeks. Eight of the 24 patients (33%) never returned to the clinic after discharge from the hospital. Follow-up was insufficient to determine bony union, nerve recovery, or elbow range of motion for the remainder of the patients.
DISCUSSION
GSWs to the elbow are challenging injuries to treat. Many factors must be considered in formulating a treatment plan, including soft tissue contamination, fracture pattern, articular involvement, the presence of nerve or vascular injury, and concomitant non-orthopedic injuries. While a relatively high number of these injuries is encountered at our level I trauma center, the overall rarity of this injury is reflected in the report by Brannon et al. [14], who described 29 GSWs to the elbow over a 10-year period.
As GSW contamination is not always apparent in the emergency department or trauma bay, the extent of surgical debridement necessary may not be known until the patient is in the operating room. All present cases underwent meticulous surgical debridement of all devitalized tissue and foreign material. Of the 24 patients treated, one was managed with staged ORIF, one required delayed definitive fixation due to preexisting deep infection and extensive fasciotomy, and 22 underwent early definitive ORIF at the time of debridement. The one staged case involved a high-velocity IIIA open fracture of the distal humerus with segmental bone loss. The surgeon determined at the time of surgery that temporary external fixation with antibiotic bead application was prudent. The patient subsequently underwent ORIF and an induced membrane technique to address the bone gap. None of the 21 cases that underwent ORIF at the time of debridement became infected. This finding suggests that early definitive fracture fixation is safe and effective in the treatment of ballistic fractures near the elbow.
Antibiotics were administered in all cases upon presentation and were discontinued within 24 hours after the last surgery. Several studies have questioned the need for IV antibiotics in the treatment of open fractures due to low-velocity GSWs [15-18]. However, since the bullet is not sterilized at the time of combustion [6,19,20] and may be a vector of infection, all ballistic fractures at our institution are managed with IV antibiotics. We typically employ a regimen of a 4th-generation cephalosporin and vancomycin. Notably, there were no cases of postoperative infection in our cohort.
The average time from presentation to surgery was just over 3 days, and in one case the patient was not cleared for surgery until 10 days after presentation. The limiting factor to orthopedic surgery was the presence of concomitant nonorthopedic injury requiring emergent surgery and/or resuscitation. These findings suggest that, in the setting of concomitant injury, surgery for an open ballistic fracture to the elbow may be safely delayed several days to allow sufficient patient stabilization and resuscitation.
Eleven patients (46%) had preoperative nerve palsy affecting the ulnar, median, and/or radial nerve. Ten of the 11 nerves were explored at the time of definitive fixation. Two of the 10 explored nerves were completely transected, while eight were in continuity. This finding confirms the contention that most nerve palsies in the context of GSWs are neuropraxic or axonotmesis but not neurotmetic injuries [21,22]. Omer [23] noted a 70% rate of spontaneous recovery in GSWs. Unfortunately, our limited patient follow-up does not allow us to comment on the rate of spontaneous recovery.
Based on the observed nerve injury patterns, our current practice is to abstain from exploring nerve injuries in the context of low-velocity GSWs to the elbow at the time of ORIF unless nerve exposure is required as part of the surgical dissection. However, we observed complete transection of the PINs in two patients with a proximal radius fracture. Although overall rates of nerve transection were low, we recommend exploration in cases of PIN palsy occurring in the context of a proximal radius fracture. Electrodiagnostic studies are not useful to distinguish between neuropraxic and axonotmetic injury [24], and we prefer to rely on serial physical examination to assess recovery. Intervention is considered if there is no noticeable improvement by 3 months after injury.
An estimated 15% of penetrating injuries to the upper extremity result in vascular injury [25]. Two patients (8%) in our cohort sustained a brachial artery injury and underwent repair. While the incidence of vascular injury is relatively low, a high level of suspicion is required due to the severity and devastating consequences of this injury. In our experience, the diagnosis of a brachial artery injury is not easy, as the patient may not present with clear signs of a dysvascular limb and distal perfusion may be present via collateral circulation. Patients with arterial injury at the level of the elbow may present in hypovolemic shock, which can lead to death [26]. When an arterial injury is present, we advocate the use of direct pressure to control hemorrhage [27]. The use of a tourniquet will compromise the collateral perfusion that is likely responsible for continued distal perfusion in cases of major arterial injury [28]. The surgical sequence of events, “fracture first” or “vascular first,” is somewhat controversial [29-31]. We prefer to proceed with rapid external fixation prior to vascular repair to protect future repair. When duration of ischemia establishes distal perfusion a priority, a temporary shunt should be applied first. Then fracture stabilization followed by definitive vascular repair can be performed.
Limitations
The limitations of this investigation emanate from the retrospective nature of the review and the low rate of postoperative patient follow-up. With the high rate of loss to follow-up, we are unable to report on long-term outcomes such as functional and patient-reported outcomes. Further, we were unable to assess long-term complications such as malunion, nonunion, or heterotrophic ossification. Inadequate follow-up remains a challenge to studies assessing this patient population. Due to this limitation, our study is primarily restricted to acute management of these injuries. Future studies should focus on capturing these long-term outcomes as they can provide better, evidence-based guidance for managing these injuries. We also lacked specific information regarding firearm type and firing range. Injuries were categorized as low-energy or high-energy except for an isolated shotgun wound; this distinction is typically sufficient for selecting a management strategy. Prospective trials comparing the timing of surgical intervention, staged versus early ORIF, and course and route of antibiotic administration are required to make definitive recommendations regarding optimal treatment strategies.
CONCLUSIONS
This investigation highlights the current management principles of ballistic fractures near the elbow at a busy urban level I trauma center. Early definitive fixation without staged debridement and intravenous antibiotic administration were utilized with results similar to those reported in the literature. The study highlights many of the commonly encountered challenges in managing GSWs near the elbow, including associated nerve injury, bone loss, and follow-up impediments in this patient population. However, quantification of the impact of these factors on overall outcome is difficult.