Comparative analysis of proximal humerus fracture management in elderly patients: complications of open reduction and internal fixation by shoulder surgeons and non-shoulder surgeons—a retrospective study
Article information

Abstract
Background
Open reduction and internal fixation (ORIF) with a locking plate is a popular surgical treatment for proximal humeral fractures (PHF). This study aimed to assess the occurrence of complications in elderly patients with PHF treated surgically using ORIF with a locking plate and to investigate the potential differences between patients treated by shoulder surgeons and non-shoulder surgeons.
Methods
A retrospective study was conducted using a single-center database to identify patients aged ≥70 years who underwent ORIF for PHF between January 1, 2011, and December 31, 2021. Data on the Neer classification, follow-up, occurrence of avascular necrosis of the humeral head, implant failure, and revision surgery were also collected. Statistical analyses were performed to calculate the overall frequency of complications according to the Neer classification.
Results
The rates of implant failure, avascular osteonecrosis, and revision surgery were 15.7%, 4.8%, and 15.7%, respectively. Complications were more common in patients with Neer three- and four-part fractures. Although the difference between surgeries performed by shoulder surgeons and non-shoulder surgeons did not reach statistical significance, the rate of complications and the need for revision surgery were nearly two-fold higher in the latter group.
Conclusions
PHF are highly prevalent in the elderly population. However, the ORIF surgical approach, as demonstrated in this study, is associated with a considerable rate of complications. Surgeries performed by non-shoulder surgeons had a higher rate of complications and a more frequent need for revision surgery. Future studies comparing surgical treatments and their respective complication rates are crucial to determine the optimal therapeutic options.
Level of evidence
III.
INTRODUCTION
Proximal humeral fractures (PHF), which constitute approximately 5% of all diagnosed fractures and exhibit a bimodal distribution, are becoming increasingly prevalent due to demographic changes. Among the elderly, PHF are the third-most common fractures and are often associated with osteoporosis [1-6].
Conservative management with short-term immobilization may be suitable for stable, minimally displaced, and displaced fractures and may yield satisfactory functional outcomes. Conservative treatment may also be appropriate for complex fractures in elderly or cognitively impaired patients, individuals with nonfunctional limbs, or those with significant medical comorbidities [7,8].
Complex fractures, including three- or four-part fractures, head-splitting, pathological, and open fractures, typically necessitate surgical management, such as open reduction and internal fixation (ORIF) with a locking plate, anterograde intramedullary nailing, or arthroplasty. Primary arthroplasty may be preferable for comminuted humeral head fractures without reconstruction options or head-split fractures and for patients older than 70 years who are at a high risk of osteonecrosis [9,10].
However, plate and screw fixation repair is associated with complications, including nonunion, implant failure/migration, osteonecrosis, infection, posttraumatic osteoarthritis, and postoperative shoulder stiffness. Reoperation may be required for implant removal due to implant failure, avascular necrosis, impingement/stiffness, pain, discomfort, or infection. Complication rates ranging from 38% to 44% have been reported in elderly patients, with reoperation rates ranging from 11% to 12% [11,12]. The majority of complications occurs within the initial 3 weeks after surgery, coinciding with the start of physical rehabilitation.
The complications and outcomes associated with different surgical treatments play a critical role in guiding treatment decisions for PHF. Therefore, this study aimed to evaluate the occurrence of complications, including the need for revision surgery, in elderly patients with PHF who underwent operative treatment with ORIF using locking plates and screws. Additionally, this study aimed to compare results between surgeons specializing in shoulder surgery (shoulder surgeons) and surgeons without specialization in shoulder surgery (non-shoulder surgeons).
METHODS
The study was approved by the Ethical Committee of Centro Hospitalar Universitário do Porto (ref. 2014.012; 10‐DEFI/012‐CES). All procedures of the study were conducted in accordance with the Declaration of Helsinki. We obtained written and verbal informed consent from all participants and/or their legal guardian(s).
This retrospective analysis focused on the surgical activities of a single orthopedic department between January 1, 2011, and December 31, 2021. The study cohort consisted of patients aged 70 years or older who underwent ORIF using the Philos locking plate (Depuy Synthes) for PHF. Data were extracted from a comprehensive single-center database and collected from medical records.
In this retrospective analysis of surgical treatments for PHF, the study cohort was stratified into two distinct categories: shoulder surgeons and non-shoulder surgeons. The shoulder surgeons group comprised patients who underwent surgery performed by orthopedic professionals from the department who were fellowship-trained with expertise exclusively in shoulder-related diagnoses, treatments, and surgical interventions. This subgroup underwent surgery performed by orthopedic surgeons with more than 5 years of dedicated experience, encompassing a diverse spectrum of shoulder-specific procedures, such as rotator cuff repairs, labral repairs, shoulder arthroscopy, proximal humerus fracture management, and shoulder replacement surgeries. These experts demonstrated an in-depth comprehension of the intricate shoulder anatomy and biomechanics, remaining well-informed about the latest advancements in shoulder surgery techniques and technologies. Conversely, the non-shoulder surgeons group consisted of patients who underwent surgery performed by general orthopedic practitioners and surgeons primarily focusing on musculoskeletal issues beyond the shoulder joint. While proficient in addressing a wide range of musculoskeletal conditions throughout the body, including shoulder-related concerns, their experience and knowledge pertaining to shoulder-specific pathologies and surgical procedures were comparatively limited.
The decision to perform surgery was based on a preoperative consensus reached by two independent surgeons who agreed that achieving a satisfactory outcome with conservative treatment was not feasible. The exclusion criteria included pathological fractures and a time interval >6 weeks from the occurrence of the fracture to the surgical procedure. All surgeries were performed successively according to rotation of the emergency department schedule. No surgery was scheduled for a particular surgeon. No patient was assigned to a specific surgeon.
All patients underwent preoperative assessments using radiography and CT. Follow-up evaluations were performed by a senior surgeon at 2 weeks, 1 month, 3 months, 6 months, and 1 year postoperative and annually thereafter. Plain radiography was performed during these follow-up visits in the anteroposterior views in neutral rotation, external rotation, and internal rotation, as well as lateral scapular shoulder or Y-views and Velpeau views. Follow-up consultations included radiographic assessments at 4 weeks, 3 months, 6 months, and 1 year, followed by annual assessments.
Demographic data were extracted from clinical records and included variables such as sex, age at the time of fracture, American Society of Anesthesiology score, Neer classification, time from fracture to surgery, visual analog scale score, duration of follow-up, mortality rate, occurrence of complications (including avascular necrosis of the humeral head and implant failure such as screw pull-out and pseudarthrosis), and the need for revision surgery.
Descriptive statistics were used to summarize the demographic data and prevalence results. For categorical variables, the number of cases and percentage were reported, and the chi-square test or Fisher’s exact test (applied when more than 20% of cells had expected frequencies less than 5 or any cell had an expected frequency less than 1.1) was used to compare the proportions between groups. Continuous variables are presented as mean and standard deviation if they followed a normal distribution or as median and interquartile range (IQR) if they did not follow a normal distribution. The Shapiro-Wilk test was used to assess the distribution of the variables, and the t-test (for normally distributed variables) or Mann-Whitney U-test (for non-normally distributed variables) was used to compare means between groups.
All statistical analyses were performed using the IBM SPSS Statistics software ver. 24.0 (IBM Corp.). Statistical significance was defined as a two-tailed P-value <0.05. When appropriate, a 95% confidence interval was reported.
RESULTS
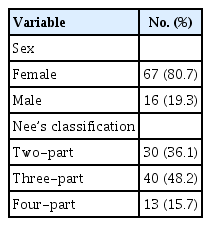
Descriptive analysis of the participants is presented in Table 1. A total of 83 participants (mean age, 77 years; range, 70–89 years) was included in the study. The mean follow-up period was 537 days (range, 370–3,841 days). According to Neer classification, 36.1%, 48.2%, and 15.7% of the patients showed two-part, three-part, and four-part fractures, respectively. The overall number of surgeons involved was 12, including four shoulder surgeons and eight non-shoulder surgeons.
Descriptive analysis
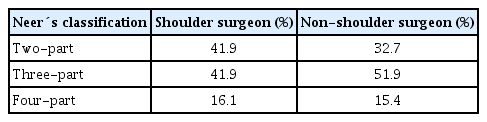
According to Neer classification, fractures treated by non-shoulder surgeons included 17 (32.7%) two-part fractures, 27 (51.9%) three-part fractures, and eight (15.4%) four-part fractures. The fractures treated by “shoulder surgeons” included 13 two-part fractures (41.9%), 13 three-part fractures (41.9%), and 5 four-part fractures (16.1%) (Table 2). No statistically significant differences in the complexity of fractures based on Neer classification were observed between shoulder surgeons and non-shoulder surgeons (P=0.590). Overall, 16.9% of the patients had complications, including avascular necrosis and implant failure in 4.8% and 15.7% of the patients, respectively. Three patients experienced both complications.
Distribution of fractures between the two groups
According to the Shapiro-Wilk test, age did not follow a normal distribution, with a median age of 76 years (IQR, 4.8 years) in the group without complications and 76 years (IQR, 4 years) in the group with complications. However, the two groups showed no statistically significant difference (P=0.643, Mann-Whitney U-test). In evaluations based on sex, 18.8% of male patients and 16.4% of female patients showed complications, with no significant sex-related difference (P=0.825).
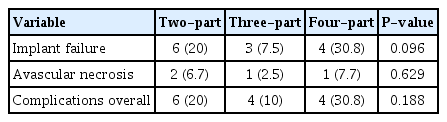
The time until surgery was also evaluated and did not follow a normal distribution, with a median time of 4 days (IQR, 5 days) in the group without complications and 2 days (IQR, 1 day) in the group with complications. The difference between the two groups was statistically significant according to the Mann-Whitney U-test (P<0.001). The frequencies of complications in relation to Neer classification (two-part, three-part, and four-part) are presented in Table 3. The differences in the frequencies of complications between Neer classes were not statistically significant (P=0.188). Difference in the frequency of complications between shoulder surgeons and non-shoulder surgeons also was evaluated; the overall frequency of complications was 21.2% in procedures performed by non-shoulder surgeons and 9.7% in those performed by shoulder surgeons. The difference between the two groups was not statistically significant (P=0.162) (Table 4).
Frequency of complications, including implant failure and avascular necrosis of the humeral head, in relation to Neer classification

Frequency of complications when patients were treated by shoulder surgeons vs. non-shoulder surgeons
The overall frequency of revision surgery was 15.7% (n=13) (Table 5). In the analyses based on Neer’s classification, two (6.7%), seven (17.5%), and four (30.8%) patients with respective two-part, three-part, and four-part fractures underwent revision surgery, with no significant difference among the groups (P=0.122). When the frequency of revision surgery was evaluated based on surgeon type, revision surgeries were required for 10 patients (19.2%) treated by non-shoulder surgeons and three patients (9.7%) treated by shoulder surgeons, although this difference was not significant (P=0.233).

Frequency of revision surgery overall, according to Neer classification, and based on surgeon type
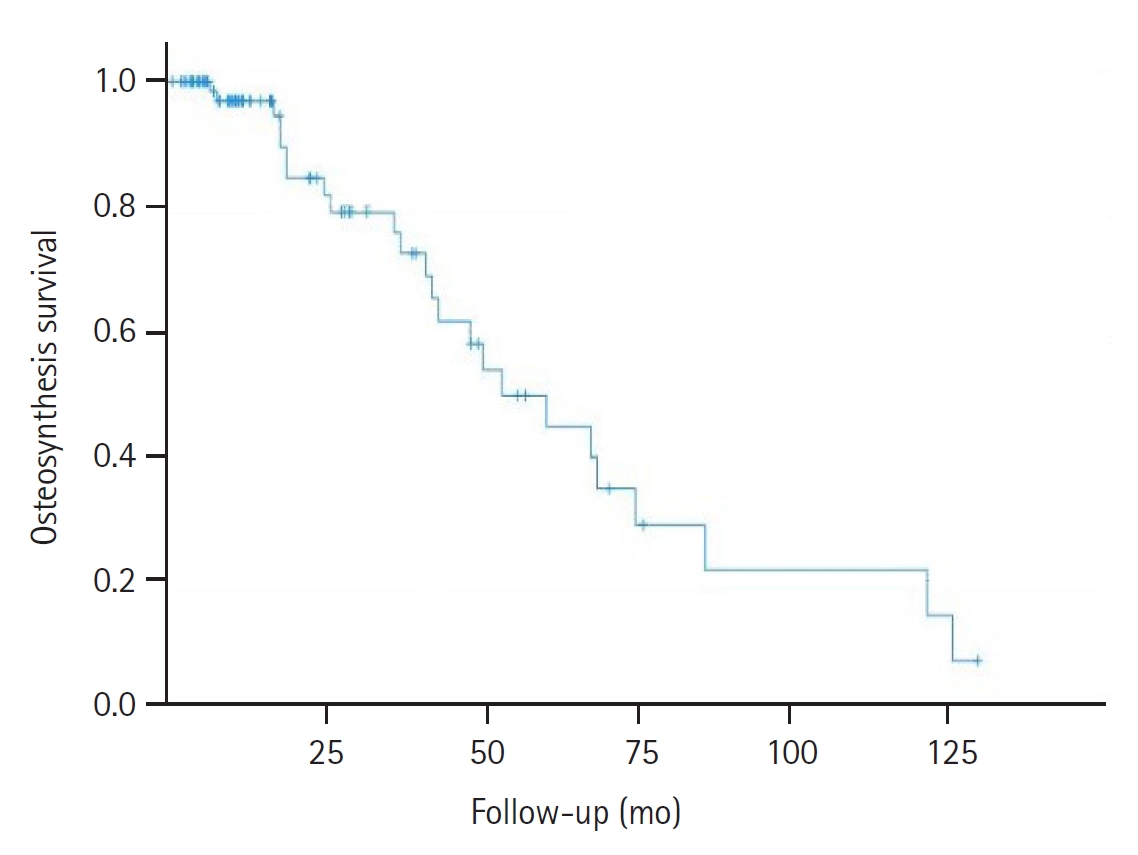
The overall implant survival rates were 82.7% at 1 year, 82.7% at 2 years, and 65.5% at 5 years (Fig. 1). During the follow-up period, 24 patients died; the overall survival rate was 96.9% at 1 year, 84.5% at 2 years, and 44.7% at 5 years (Fig. 2).
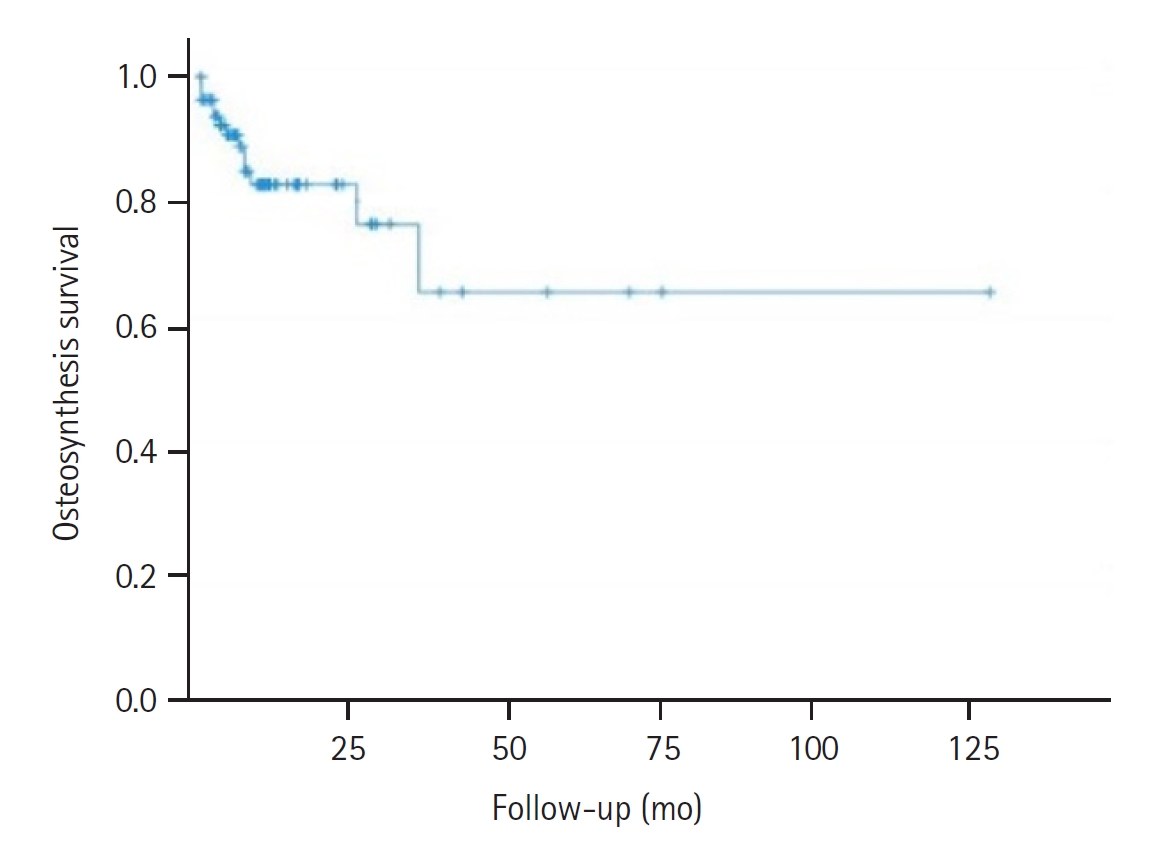
Implant survival rate.
Mortality rate.
DISCUSSION
This study provides valuable insights into the management of PHF in elderly populations, which remains a challenge, and treatment approaches show substantial variations across regions. The rates of surgical interventions for PHF also display significant variability, highlighting the absence of a consensus regarding the optimal approach to these fractures [13].
The findings highlight the high rate of radiographic failure and reoperation following ORIF for PHF, particularly in cases treated by non-shoulder surgeons. The greater success of shoulder surgeons could be attributed to their enhanced expertise within this specific anatomical domain and their use of surgical techniques designed to minimize the risk of vascular injuries, mitigating the potential for avascular necrosis. It is also conceivable that their greater familiarity with precise fracture reduction and screw placement aids in preventing substantial reductions due to slipping. The reduced occurrence of complications among specialists in this field may also stem from their notably shorter surgical durations owing to their extensive knowledge of shoulder anatomy. Existing literature on ORIF for PHF has identified several variables associated with successful radiographic outcomes. Achieving anatomic reduction and restoring the calcar have been shown to decrease the incidence of complications such as varus collapse, nonunion, malunion, and screw cutout [14-16]. These factors play crucial roles in determining the long-term stability and functional outcomes of patients with PHF.
The survival rate of this specific population, consisting of individuals aged >70 years in our study, highlighted the notable longevity of these patients. Consequently, from the perspective of enhancing the patients’ quality of life, well-informed decision-making regarding treatments that effectively address the fracture are crucial.
Regrettably, the incidence of complications following ORIF for PHF has consistently remained elevated. Recent studies have reported complication rates at the 2-year mark ranging from 20% to 60% [17]. Among the most frequently encountered complications associated with proximal humerus plating are screw cutouts and intra-articular screw complications, tuberosity displacement or non-union, impingement, rotator cuff lesions, malunion or non-union, secondary displacement, osteonecrosis of the humeral head, posttraumatic osteoarthritis, screw loosening, heterotopic ossification, infections, and implant failure [17]. Several risk factors have been identified as contributors to these complications following ORIF for PHF, shedding light on patients who may be at a higher risk. These risk factors encompass fracture-dislocations, smoking, obesity, advanced age, and the presence of comorbidities [18,19]. Notably, specific factors associated with an increased risk of osteonecrosis include fracture-dislocation, disruption of the medial hinge (calcar), and limited metaphyseal head extension (<8 mm) [20]. Furthermore, the risk of screw cutout is amplified in cases involving advanced age, non-anatomic calcar reduction, fracture-dislocation, and fractures falling within the AO/OTA 11-C2 category (impressed fractures with significant displacement) [21].
Fracture complexity is expected to be associated with increased complication rates and need for revision surgeries, although this trend did not reach statistical significance in the present study. In our study, when comparing surgeries performed by shoulder surgeons and non-shoulder surgeons, the latter group showed a nearly two-fold higher rate of complications and revision surgeries. This difference was particularly notable in terms of implant failure rates, suggesting that dedicated shoulder surgeons are more likely to avoid complications and reoperations in this specific patient population.
A previous study reported reoperation rates of 11% and 2.2% in hemiarthroplasty and reverse shoulder arthroplasty groups, respectively [22]. Our study's radiographic failure rate of 16.9% and reoperation rate of 15.7% compared with the arthroplasty option indicated worse radiological outcomes. This comparison suggests that ORIF for PHF in elderly patients may result in higher complication and recurrence rates than arthroplasty. Another significant finding was that fractures with a higher Neer classification were prioritized for earlier surgical intervention. This trend indicates a tendency among orthopedic surgeons to address more complex cases promptly, potentially mitigating the risk of complications such as avascular necrosis.
This study had some limitations. The retrospective design inherently restricted the establishment of causal relationships and forced reliance on correlational findings. Additionally, the relatively rare occurrence of ORIF for PHF in this specific elderly population resulted in a small sample size, potentially limiting the ability to detect significant differences in failure rates and functional outcomes. Furthermore, the involvement of 12 surgeons with varying levels of experience introduced potential variations in the surgical techniques and rehabilitation protocols. Despite these limitations, our analysis underscores the notion that, even with well-reduced fractures, the elderly patient population undergoing ORIF for PHF does not achieve robust radiological outcomes.
CONCLUSIONS
The results of this study highlight the considerable incidence of complications and the increased likelihood of reoperation associated with ORIF procedures for PHF in the elderly population, particularly when performed by non-shoulder surgeons. In cases where satisfactory fracture reduction is challenging, arthroplasty may be a more favorable alternative.
These findings emphasize the critical importance of meticulous surgical techniques and appropriate patient selection to optimize outcomes in patients with PHF, especially for patients in the elderly population. Recognizing the expertise of dedicated shoulder surgeons is crucial to achieve better results and minimize complications.
Additional research is imperative to explore innovative approaches and advance management strategies for PHF. Future studies should focus on refining the surgical techniques, developing patient-specific treatment algorithms, and investigating the role of arthroplasty options in specific fracture patterns and patient populations. Continued research efforts and concurrent changes in clinical practice will contribute to improving the outcomes of elderly patients with PHF and providing optimal care for this patient population.
Notes
Author contributions
Conceptualization: RC. Data curation: RC, BB, CF. Formal analysis: RC, BB, CF, AR, LHB. Methodology: AR. Project administration: RC. Software: A Ribau. Supervision: RC. Validation: RC, BB, CF, AR, LHB. Visualization: AR. Writing – original draft: RC. Writing – review & editing: RC, AR, LHB.
Conflict of interest
None.
Funding
None.
Data availability
Contact the corresponding author for data availability.
Acknowledgments
The authors would like to thank the participants for their cooperation, and they also greatly appreciate the assistance of the staff members who were involved in this study.