INTRODUCTION
Total elbow arthroplasty (TEA) is a relatively uncommon and complicated surgery. Although it was first designed to treat rheumatoid arthritis of the elbow, indications for TEA have since expanded to include inflammatory arthritis, osteoarthritis, and post-traumatic arthritis, as well as complex, unreconstructable distal humerus fractures [1].While far less common than total knee and hip arthroplasties, the number of TEA procedures performed in the United States continues to increase each year, placing a greater burden on the healthcare system [2].
One method of minimizing this increasing burden is transitioning to an outpatient setting. Studies have documented significant reductions in cost with outpatient total joint arthroplasties [3,4]. Total hip, knee, and shoulder arthroplasties have all proven safe and feasible in this setting [5,6], and projections predict that over half will be outpatient procedures by 2026 [7]. Moreover, recent data on TEA show that outpatient surgery results in decreased costs for patients [8]. While the majority of TEA procedures remain inpatient, from 2010 to 2017, the proportion of TEAs performed outpatient increased from 2.4% to 34.5% [9].
As the proportion of outpatient TEA procedures increases, it is important to monitor the outcomes resulting from this new practice pattern. The aim of this study is twofold: to characterize the patient populations undergoing inpatient and outpatient TEA, respectively, and to compare 30-day outcomes between operative settings. We hypothesize that there will be no apparent differences in these aspects of TEA between inpatient and outpatient settings.
METHODS
This study did not require institutional review board review nor informed consent as ACS NSQIP is a pre-existing, deidentified dataset and is not considered human subjects research.
Data Source and Collection
Data were drawn via a retrospective analysis of the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. The ACS NSQIP is a multi-institution, multi-center database that collects >270 patient variables from procedures performed at >500 hospitals. Trained clinical reviewers at each site input preoperative, intraoperative, 30-day postoperative, and discharge data based on the patientŌĆÖs Current Procedural Terminology (CPT) code. This dataset is subject to routine audits for quality assurance. We used CPT codes to identify all adults (patients >18 years of age) who underwent TEA between 2016 and 2020. Patients with incomplete records or with concurrent procedures were excluded.
To isolate the impact of surgical setting, we collected a number of preoperative variables to account for any baseline differences in the two patient populations. We collected the following patient characteristics: demographics, including age, sex, race, and ethnicity; smoking history; American Society of Anesthesiologists class; and common comorbidities such as liver disease, chronic obstructive pulmonary disorder (COPD), diabetes, congestive heart failure, hypertension, and dialysis-dependent kidney disease. Body mass index (BMI) was calculated from patient height and weight.
To assess outcomes, we collected postoperative medical complications within 30 days, including pneumonia, pulmonary embolism, cerebrovascular accidents, deep vein thrombosis, acute renal failure, urinary tract infection, cardiac arrest, and myocardial infarction. We also collected information on both superficial and deep surgical site infections, wound class, blood transfusions, reoperation within 30 days, operation time, hospital length of stay, and discharge disposition. Adverse discharge was defined as patient discharge to any location or facility other than their home.
Statistical Analysis
Patients were stratified based on procedure setting (inpatient or outpatient). Data were analyzed to ensure assumptions were met for statistical analysis. For normally distributed data, independent sample t-tests were performed, while the Wilcoxon rank-sum test was used for non-normally distributed data. Categorical variables were assessed with FisherŌĆÖs exact test or chi-square with Kendall tau test. Multiple linear and logistic regression models were also analyzed to ensure criteria were met. Perioperative outcomes with P<0.05 after multivariate regression were considered significant, and results were reported as adjusted odds ratio (OR) and 95% confidence interval (CI).
Statistical analysis was performed with the IBM SPSS ver. 28.0.1.0 (IBM Corp.). Power analysis was conducted with the University of California Los AngelesŌĆÖ Advanced Research Computing Statistical Methods and Data Analysis G*Power Statistics tool. CIs were set at 95%, with P=0.05 being considered statistically significant.
RESULTS
Demographics
A total of 468 patients, representing 303 inpatient and 165 outpatient procedures, was included in our analysis. In the entire study sample, the average patient age was 67┬▒13 years, with a mean BMI of 29.64┬▒7.18 kg/m2. A total of 379 patients (79.1%) were female, 25 (5.3%) were Black, and 55 (11.8%) were Hispanic. There was no significant difference in mean age (P=0.908) or BMI (P=0.870). The mean length of stay for the inpatient cohort was 3.5 days (standard error [SE], 0.24 days), while the outpatient cohort had a mean length of stay, by definition, of 1 day. The mean operation time was not significantly different at 163 minutes (SE, 3.83 minutes) for the inpatient cohort compared to 160.7 minutes (SE, 5.04 minutes) for the outpatient cohort (P=0.708).
Postoperative Outcomes
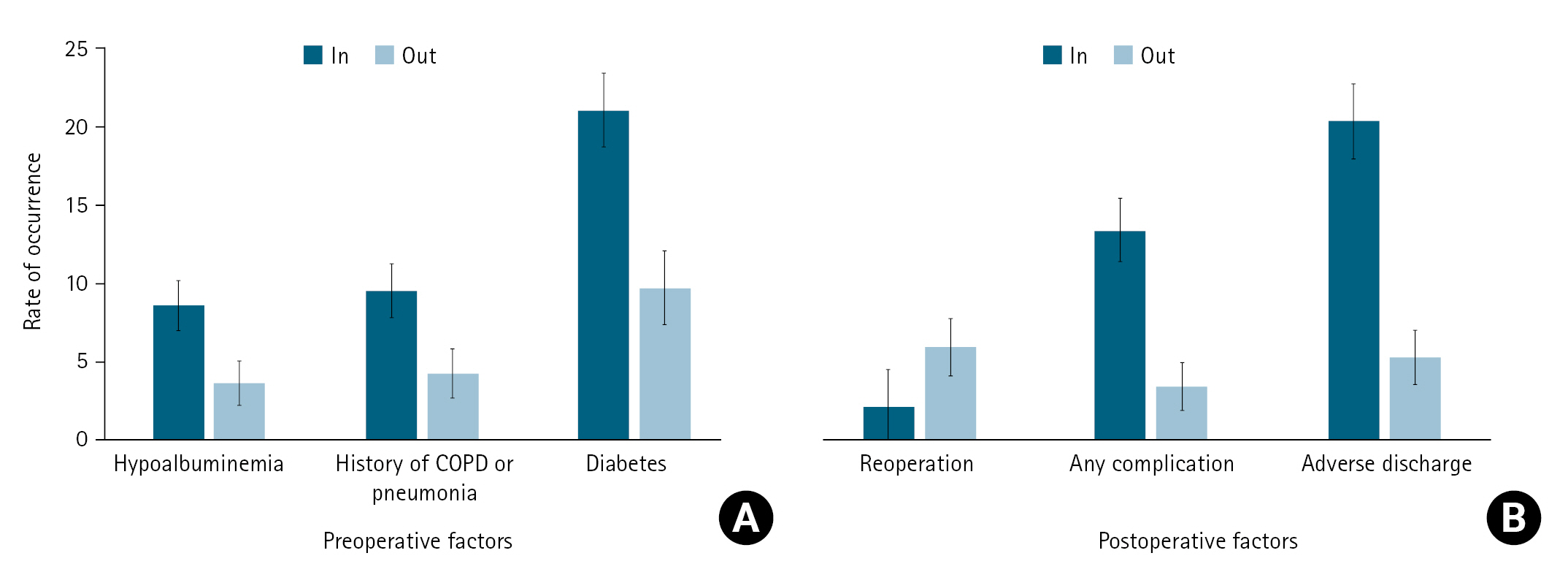
After controlling for age, sex, ethnicity, race, and BMI through multivariate regression, we found those undergoing an inpatient procedure to be more likely to have a complication (OR, 4.1; 95% CI, 1.7ŌĆō9.9; P<0.001) or an adverse discharge disposition (OR, 4.5; 95% CI, 2.2ŌĆō9.2; P<0.001) but less likely to require reoperation (OR, 0.4; 95% CI, 0.1ŌĆō0.9; P=0.037) compared to patients undergoing an outpatient procedure. These results can be seen in Figs. 1 and 2.
Preoperative Factors Associated with Inpatient Status
At baseline, those undergoing an inpatient procedure were more comorbid; specifically, we found that patients undergoing an inpatient procedure were more likely to have hypoalbuminemia (OR, 2.5; 95% CI, 1.0ŌĆō6.2; P=0.029), history of COPD or pneumonia (OR, 2.4; 95% CI, 1.0ŌĆō5.6; P=0.029), or diabetes (OR, 2.5; 95% CI, 1.4ŌĆō4.5; P=0.001) relative to patients undergoing outpatient procedures. These results can be seen in Figs. 1 and 2.
DISCUSSION
We found that hypoalbuminemia, a history of COPD or pneumonia, and a diagnosis of diabetes mellitus were more prevalent in the inpatient TEA population. We also found that inpatient TEA is associated with increased odds of both complications within 30 days and adverse discharge but lower odds of reoperation. These data can aid surgeons in selecting both the operative setting and patients by providing a greater understanding of the risks involved.
Increased rates of both complications and adverse discharge in the inpatient population have been reported previously in TEA-specific studies [10] and studies on other total joint operations [5] alike. Our study provides further evidence of this trend. Furthermore, we identified specific patient characteristics and comorbidities that significantly increased the odds of an inpatient TEA procedure, which, to our knowledge, has not been done previously.
While Furman et al. [10] found no difference in TEA reoperation rates, increased reoperation rates in outpatient total joint arthroplasty have been reported [11]. Arshi et al. [12] obtained similar findings for shoulder arthroplastiesŌĆöthat is, reoperation rates are higher following outpatient procedures, typically due to postoperative infections. Although outpatient surgery is typically associated with significant savings, the increased rate of reoperations could make it a less cost-effective option [8,13]. Better patient selection, guided by studies such as our own, may also minimize the disparity in reoperation rates.
While Arshi et al. [12] found that reoperation due to surgical site infection was more common in the outpatient population, other studies suggest that infection rates are not significantly different between surgical settings [14]. TEA-specific studies have reported relatively high reoperation rates (up to 41%), often attributed to complications such as component loosening and periprosthetic fracture [15-17]. However, in these studies, the average time to reoperation ranged from 1.8 to >7 years. As our analysis was restricted to 30 days postoperatively, our results suggest that this discrepancy in reoperation rates is due to acute complications, such as wound infection. Therefore, better infection control may mitigate these observed differences. However, further research comparing longitudinal reoperation rates is warranted.
With respect to complications, generally, outpatient TEA has proven to be safe and produce reliable outcomes; however, we recorded significantly more complications resulting from inpatient surgery. Several studies found no difference in inpatient and outpatient complication rates; however, those studies had limitations [10,18,19]. Stone et al. [18], although they tracked complications out to 90 days, enrolled only 28 patients. The study by Albert et al. [19] was restricted to procedures performed by a single surgeon with changing practice patterns over the 18 years of perioperative data included in the study, limiting the generalizability of its findings. However, Furman et al. [10] reported results consistent with our own: greater surgical and medical complications in the inpatient setting. However, while their study had a sample size comparable to our own and a robust statistical analysis, our study drew data from more recent years; therefore, these differences are likely the result of changes over time.
We also found that the inpatient cohort had a significantly greater comorbidity burden. Specifically, our results indicate that hypoalbuminemia, COPD or pneumonia, and diabetes mellitus are associated with increased odds of an inpatient TEA procedure. Hypoalbuminemia, a sign of malnutrition, has been found to predict postoperative complications, longer hospital stays, and mortality after hip fracture repair [20]. It is also associated with postoperative complications and mortality after outpatient surgery [21]. In a related study on total shoulder arthroplasty, Mehta et al. [22] found that patients undergoing outpatient procedures were less likely to have hypoalbuminemia, further supporting this association. COPD is also associated with postoperative complications after both total hip and knee arthroplasty [23,24]; specifically, COPD patients were at increased odds of developing pneumonia, undergoing unplanned intubation, and requiring ventilator support for >48 hours within 30 days of the arthroplasty procedure.
With respect to diabetes mellitus, J├żmsen et al. [25] found hemoglobin A1c (HbA1c) concentration to be an accurate predictor of perioperative hyperglycemia; nearly all patients with an HbA1c concentration Ōēź6.5% (a level indicating diabetes) in their study experienced hyperglycemia after hip and knee arthroplasty. Post-arthroplasty hyperglycemia is associated with increased wound complications and mortality [26]. Brophy et al. [27] found that diabetes was associated with postoperative infection in the outpatient setting; our findings indicate that surgeons are more likely to opt for an inpatient procedure with these patients. While A1c and blood sugar are important considerations when selecting candidates for outpatient surgery, proper glycemic control in diabetic patients can bring postoperative complication rates in line with those among patients without diabetes [28].
All of these characteristics are associated with increased complications and mortality after total knee and hip arthroplasty. Hypoalbuminemia, history of COPD, and uncontrolled diabetes are all considered possible exclusion criteria for outpatient total hip and knee arthroplasty [29]. Our results show that surgeons are also wisely electing to perform TEA in a setting where these patients can benefit from close postoperative monitoring. This represents the existence of a significant patient population that is limited in its access to outpatient total joint arthroplasty due to the inherent risk of complications. Future research into pre- and post-arthroplasty risk mitigation for patients with these characteristics would improve patient safety and eventually open the door for cost-saving outpatient arthroplasty.
Our findings of greater comorbidity burden in the inpatient population are consistent with findings by Guareschi et al. [30], who found that patients undergoing inpatient shoulder arthroplasty had higher American Society of Anesthesiologists class scores relative to those undergoing outpatient procedures. These higher-risk patients with more comorbidities tend to require the more intense postoperative care offered in an inpatient setting. However, our results suggest that optimizing pre-operational patient nutrition status, identifying pulmonary function parameters that predict postoperative complications, and ensuring proper glycemic control could expand eligibility for outpatient TEA, allowing a subgroup of this traditionally inpatient population to potentially transition safely to outpatient arthroplasty.
Our study benefits from including a far larger sample size than most other extant studies. The ACS NSQIP provides cross-country sampling, allowing us to draw conclusions that should be generalizable across the United States. Additionally, we had access to numerous patient variables and demographic information, allowing us to control for key factors (common comorbidities, age, race, and BMI) that can influence outcomes. These data are important for surgeons to appropriately select candidates for outpatient surgery.
As with any study, ours has several limitations. First, this was a retrospective study, not a randomized controlled trial. Second, the ACS NSQIP, while it allows for an exceptionally large sample size representative of the country, lacks several key variables, such as patient-reported outcomes, functional outcomes, long-term outcomes, and complications beyond 30 days. We also lacked information on variables and complications specific to TEA procedures, such as aseptic loosening, ulnar neuropathy, or the different forms of prosthesis wear and failure, and were unable to account for important patient characteristics like insurance and socioeconomic status, which may have significant impacts on outcomes. Further research on these orthopedic-specific outcomes and complications is warranted.
CONCLUSIONS
Hypoalbuminemia, COPD or pneumonia, and diabetes mellitus are significantly more prevalent in the inpatient TEA population. These patients are more comorbid and warrant the increased level of care offered with inpatient surgery. Notably, while inpatient TEA is associated with greater odds of complications and adverse discharge, it lowers the odds of reoperation. Our findings suggest that outpatient TEA is generally safe and a viable option; however, patients with a greater comorbidity burden are preferentially treated in the inpatient setting. Further research is warranted to optimize patient selection in the outpatient setting and potentially to realize significant cost savings.