INTRODUCTION
Shoulder instability is a very common complaint among the general population. Depending on the nature and intensity of the dislocation/subluxation event, instability may manifest as anterior, posterior, or multidirectional [1-3]. Anterior instability is the most common [1-3]. Contact sports, young age, joint hypermobility, and previous dislocation events are all common risk factors for shoulder instability [4,5]. The incidence of anterior shoulder instability is thought to be 0.08 per 1000 person-years in the general population, with rates of 3% per year in young, high-risk males [6,7]. Treatment methods range from conservative interventions to surgical procedures [3]. However, in younger high-risk patients, surgical intervention is often advised after the initial dislocation to prevent future dislocations and concurrent bone loss [3].
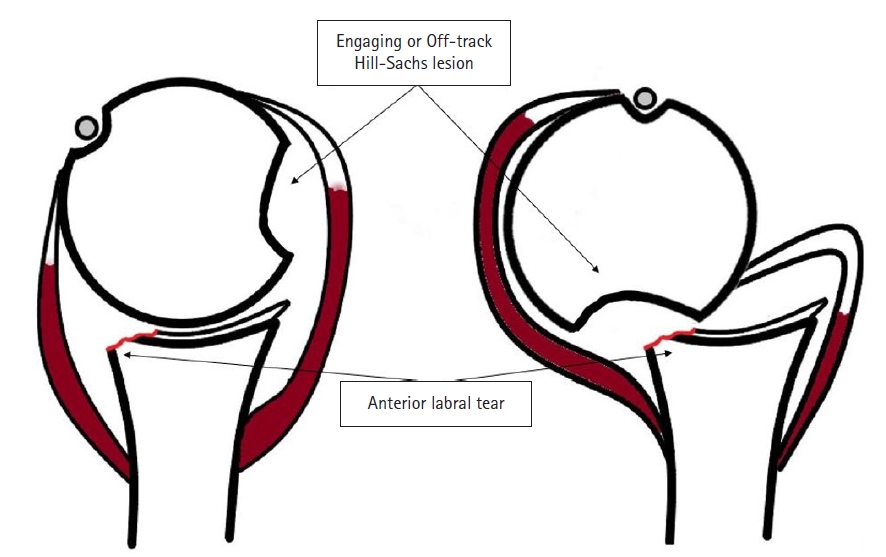
In an anterior glenohumeral dislocation, the dense cortical glenoid bone presses against the softer cancellous bone of the posterosuperior humeral head. This bone contact causes a defect in the humeral head commonly known as a Hill-Sachs lesion (HSL), which was originally identified in 1940 [8]. HSLs play a significant role in the recurrence of glenohumeral instability [8,9]. To help identify lesions that are key causes of instability, the âengagingâ HSL was described as one that engages the rim of the glenoid when the shoulder is abducted and externally rotated, resulting in joint locking and instability (Fig. 1) [10,11].
Many techniques have been suggested to treat posterosuperior humeral head defects, such as humeral head osteotomy, anterior capsular plication, osteochondral allograft, humeroplasty, and limited resurfacing arthroplasty [12-19]. Despite the likelihood of good clinical outcomes, these procedures typically involve an open approach and have risks of infection, implant failure, nonunion, and glenohumeral arthritis [12-19]. One modern technique that addresses this defect involves a capsulo-tenodesis in which the infraspinatus tendon and posterior capsule fill the HSL to prevent it from contacting the glenoid [20]. This technique, termed the remplissage, was first described in 2004, and has since generated growing interest for its ability to manage critical HSLs [20-24]. Many surgeons favor the remplissage over arthroscopic Bankart repair alone for its potential to lower rates of recurrent instability. However, the use of tenodesis in the remplissage procedure introduces the risk of reduced postoperative range of motion (ROM) [25].
Exploring the current literature can provide a holistic view of a certain techniqueâs efficacy. The remplissage has recently garnered increasing attention for its positive outcomes and low complication rates. Its addition to the arthroscopic Bankart repair produces comparable outcomes to those of the Latarjet procedure in some populations. To confirm this utility, the objective of this review was to explore the history, indications, and clinical and patient-reported outcomes of the remplissage technique.
HISTORY
The first report of humeral head defects in unstable shoulders occurred in the 1800s, when Flower described a groove located posterior to the greater tuberosity during his dissections [26,27]. Later, between the late 1800s and early 1900s, several case reports provided additional descriptions of the posterior articular lesion [27]. In 1940, Hill and Sachs [8] described the lesion as an impact injury that causes a groove on the posterolateral articular surface of the humeral head. The mechanism of injury was defined as posterolateral impingement of the humeral head on the glenoid rim, which often occurs during anterior glenohumeral dislocation. In 1972, Connolly [28] described an open transfer technique during which the infraspinatus tendon was used to fill the HSL. This technique was analogous to the McLaughlin procedure and converts the HSL into an extra-articular lesion, which protects the humeral head from gliding over the glenoid rim [28]. Many different techniques have since been proposed to treat critical HSLs, including open capsular shift, partial resurfacing, osteochondral allograft transplantation, and transhumeral head plasty [12-19].
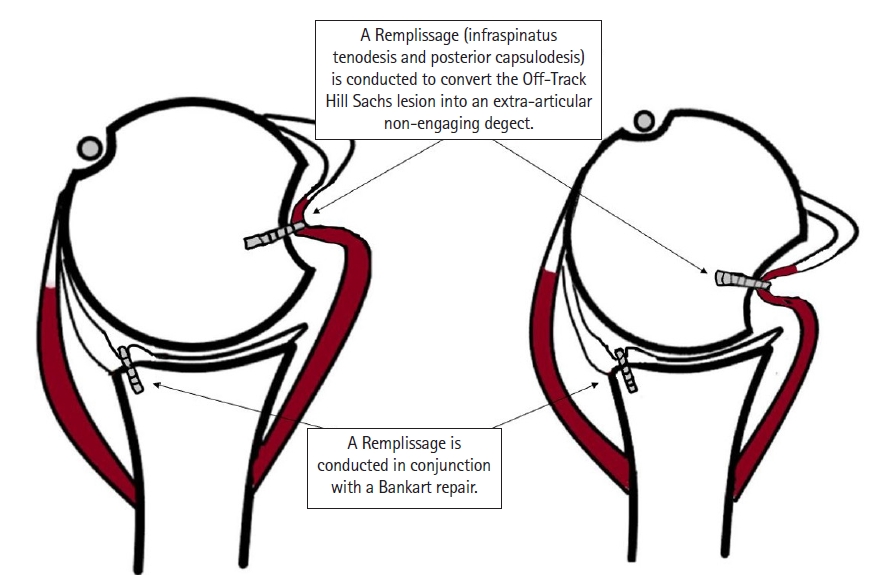
The arthroscopic remplissage, which in French means âto fill,â was described by Wolf and Pollack [24] in 2004. The technique converts the HSL into an extra-articular lesion by conducting posterior capsulodesis and infraspinatus tenodesis onto the humeral head defect (Fig. 2). This procedure decreases anterior glenohumeral translation and protects against impact of the glenoid rim with the humeral head [24]. Numerous studies have described positive results when the remplissage is performed in conjunction with the arthroscopic Bankart repair. Some have reported comparable clinical outcomes of the remplissage and Bankart repair to those after robust open procedures like the Latarjet [27,29-32]. Since its development, the remplissage has gained notable attention, with numerous publications exploring its clinical and surgical utility.
INDICATIONS
Several clinical factors are considered regarding the use of the remplissage in the management of anterior shoulder instability, including the size of the glenoid bony defect, the size of the HSL, and most importantly, the location of the HSL in regard to the glenoid. Thus, the glenoid track concept was presented to evaluate the risk of HSL in relation to the glenoid [33,34]. The glenoid track is the region of the posterior humeral articular surface that comes into contact with the glenoid when the arm is externally rotated and abducted. There is minimal risk of an HSL engaging or dislocating with the anterior rim of the glenoid if the medial border remains within the glenoid track. However, if the HSL extends beyond the medial edge of the glenoid track, the HSL may exit the glenoid track and cause a new dislocation (Fig. 1) [35]. The former scenario has been referred to as a ânon-engaging HSLâ and the latter as an âengaging HSL.â However, the new terminology is âon-track HSLâ and âoff-track HSLâ [36].
The remplissage is often indicated for an âoff-trackâ HSL with a minimal to moderate glenoid bony defect. However, there has been debate regarding the extent of glenoid bony defect or HSL size suitable for a remplissage [27]. One retrospective cohort study comparing remplissage to modified Latarjet showed on multivariate analysis that glenoid bone loss >10%â15% may be a risk factor for recurrent postoperative instability following remplissage in patients with off-track HSL [37]. However, a biomechanical study by Garcia et al. showed that this surgical technique can be used with glenoid bone loss up to 17% and an HSL reaching 30%. Some researchers have suggested that the remplissage should be avoided in HSL that affected >20% of the humeral head [38,39]. Degen et al. [30] reported in a biomechanical study that remplissage and Latarjet had similar outcomes in treating HSLs up to 25% of the humeral head without affecting joint stiffness. Finally, a meta-analysis performed by Haroun et al. [40] showed no difference in recurrence, patient outcomes such as visual analog scale (VAS) and Rowe score, or ROM between the Latarjet and remplissage in the treatment of glenoid defects <20% and HSL involving 20%â30% of the humeral head.
A patientâs lifestyle, including sports and activities, is an important factor to consider when selecting the appropriate surgical intervention for anterior instability. Although the overall return to sport (RTS) rate after the remplissage has reached 95%, the rate was only 51%â65% for overhead throwing athletes [41]. Ding et al. [42] explored possible reasons why external rotation can be limited following remplissage and showed that it was correlated with the placement of the medial anchor. This potential risk is important to address when remplissage is considered in patients who are overhead throwing athletes.
CLINICAL OUTCOMES
Patient-Reported Outcomes
Numerous studies have explored the clinical outcomes of the remplissage in patients with anterior shoulder instability. Martinez-Catalan et al. [43] described 43 patients treated with arthroscopic Bankart repair and remplissage for bipolar glenoid bone defects with <20% glenoid bone loss. At a minimum 4-year follow-up, the mean Walch-Duplay score was 87.9 and the mean Rowe score was 93.7. A systematic review by Lazarides et al. [22] examined clinical and biomechanical studies describing arthroscopic remplissage for patients with off-track HSLs. The group included studies of patients with nonsignificant or unsubstantial (in three studies) glenoid bone loss, less than 20% (in five studies) bone loss, and less than 25% (in nine studies) bone loss [22]. The authors reported significant improvements in mean postoperative patient reported outcomes for all studies, with only 5.8% of total shoulders displaying recurrent instability postoperatively [22]. In contrast, studies of patients with higher degrees of instability and bone loss have shown conflicting results. Brejuin et al. [44] explored the outcomes of 51 patients who underwent arthroscopic Bankart repair with remplissage for anterior shoulder instability and off-track HSLs. The patients had a mean age of 26 years, and 70% of them reported participation in sports. At a minimum 5 years of follow-up, patients had a mean Rowe score of 88, a Walch-Duplay score of 82, and a subjective shoulder score (SSV) of 89. Nevertheless, 15.6% of patients, mainly those with larger HSLs, had recurrent subluxations or dislocations [44]. This finding prompted the authors to advise caution when performing the procedure in patients with more severe lesion [44].
Several studies have compared arthroscopic Bankart repair with remplissage to other procedures for anterior instability. Han et al. [45] performed a retrospective study comparing the outcomes in patients who underwent arthroscopic Bankart repair with remplissage to those who underwent the reverse McLaughlin procedure for engaging HSLs and anterior shoulder instability at a single institution. At an average of 16.8 months of follow-up (range, 12â34 months), patients in the two groups had similar clinical outcome scores with no significant differences in preoperative or postoperative American Shoulder and Elbow Surgeons (ASES) score, Constant scores, 36-item short form survey (SF-36) physical component summary score, or SF-36 mental component summary score [45]. Another retrospective review by Hurley et al. [46] showed no difference in outcomes after arthroscopic Bankart repair with remplissage compared to arthroscopic Latarjet for patients with anterior shoulder instability with a labral tear and engaging HSL. The groups had similar preoperative measurements with the exception of glenoid bone loss [46]. The remplissage group had 7.3% (Âą7.8%) glenoid bone loss, while the Latarjet group had 19.1% (Âą4.7%, P<0.0001) [46]. At a minimum follow-up of 24 months (mean follow-up: 58.5 months for remplissage group vs. 52 months for Latarjet group), the outcome score averages were as follows: Western Ontario Shoulder Instability Index (WOSI) score of 21.8% vs. 28.2% (P=0.329), VAS score of 0.9 vs. 1.4 (P=0.317), VAS score for sport of 1.7 vs. 2.4 (P=0.29), SSV of 78.4 vs. 74.5 (P=0.606), SIRSI of 69.3 vs. 62.8 (P=0.337), rate of satisfaction of 81.6% vs. 85.6% (P=0.54), and willingness to repeat prior surgery of 81.6% vs. 96.1% (P=0.16) for the remplissage and Latarjet groups, respectively. Both groups had 100% return to work rates [46].
When comparing arthroscopic Bankart repair with remplissage to the Latarjet for patients with off-track Hill-Sachs and subcritical glenoid bone loss, Horinek et al. [47] hypothesized that the procedures would achieve comparable results for patients with greater than 15% glenoid bone loss. In their multicenter retrospective study, the authors explored the outcomes of 47 patients (22 patients in the remplissage group and 25 patients in the Latarjet group) with similar preoperative clinical and demographic characteristics [47]. The authors reported excellent outcomes in both groups: mean Single Assessment Numeric Evaluation (SANE) improvement of 38.8 in the Latarjet group versus 36.4 in the remplissage group; mean VAS improvement of 1.9 in the Latarjet group versus 2.0 in the remplissage group, and mean WOSI improvement of 1,092.3 in the Latarjet group versus 1,173.5 in the remplissage group [47]. Yang et al. [37] reported similar findings but noted conflicting results in the setting of revision surgery and in injury severity. In a retrospective review of 189 patients at two surgical centers, 98 were in the remplissage group and 91 in the modified Latarjet group [37]. At a mean follow-up of 3.2 years (range, 2â12 years), the remplissage group and modified latarjet group had similar WOSI scores (411 vs. 352, P=0.164), SANE scores (86.8 vs. 88.1, P=0.111), revision rates (16% vs. 6%, P=0.078), and recurrent instability (13% vs. 5%, P=0.085) [37]. Patients in the remplissage group had a significantly higher VAS pain score than those in the Latarjet group (2.2 vs. 1.55, P=0.041), while patients in the Latarjet group had higher complication rates than those in the remplissage group (1% vs. 12.1%, P=0.002) [37]. Using univariate analysis to compare subgroups, the authors saw higher VAS scores (3.6 vs. 2.2, P=0.001), recurrence rates (34.8% vs. 10.3%, P=0.42), and revision rates (43.5% vs. 15.4%, P=0.019) in the remplissage group than in the Latarjet group for patients undergoing revision surgery [37]. In the collision athlete subgroup, the remplissage group had worse WOSI scores (138 vs. 231, P=0.019) and higher recurrence (30 vs. 0, P=0.005) than the Latarjet group [37].
Range of Motion
Since the remplissage is a non-anatomical procedure to restore shoulder joint stability, an inevitable consequence is loss of ROM [31,32,41]. Several studies have evaluated the degree of limitation and how it compares to the results of other shoulder-stabilizing surgeries, with varying results. In the previously mentioned cohort study by Yang et al. [37], the authors compared the ROM between patients who underwent Bankart repair with remplissage to those who underwent a modified Latarjet procedure for off-track HSLs with <25% glenoid bone loss. At a minimum follow-up of 2 years after surgery, the ROM was generally comparable between the two groups without any significant differences, except in internal rotation in abduction, where the remplissage group had 12.3° greater limitation than did the Latarjet group (40.9° vs. 53.2°, P=0.006) [37]. This difference was attributed to the tenodesis of the rotator cuff. Bastard et al. [48] showed in their retrospective comparative study that Bankart repair with remplissage had a higher overall Walch-Duplay score (91.4 vs. 83.8, P<0.05) and higher mobility-specific Walch-Duplay score (22.8 vs. 17.4, P<00.01) compared to Bankart repair alone at the 10-year follow-up. This study focused on patients who had recurrent shoulder instability with a dynamic off-track HSL and no prior shoulder stabilization surgeries [48]. The improved mobility scores for the Bankart repair with remplissage could be attributed to the overall improvement in shoulder function [48].
Brilakis et al. [49] evaluated 51 patients who underwent Bankart repair with remplissage for off-track HSLs and <25% glenoid bone loss. This group compared preoperative and postoperative ROM at 2 years of follow-up. The authors reported postoperative increase in active forward flexion (+10°) and external rotation at 0° of abduction (+6°), a decrease in external rotation at 90° of abduction (â3°), and no change in internal rotation; however, none of these values were significant. A subjective difference in external rotation compared to the contralateral shoulder was reported in 14% of patients. However, there was no associated limitation in daily or sporting activities, and the measured difference between the two shoulders was less than 10°. These findings complement those of Lazarides et al. [22] who noted that external rotation in the neutral arm position was the most limited ROM parameter after arthroscopic remplissage, with a deficit of 9°â14° in the operated shoulder compared to the contralateral shoulder.
A 2020 retrospective cohort by Pandey et al. [50] compared patients who underwent Bankart repair alone with those who underwent Bankart repair with remplissage at a minimum follow-up of 2 years. They found significantly greater loss of ROM in the remplissage group, with a 3.4° difference in external rotation at adduction (15.3°¹7.2° vs. 18.7°¹10.1°, P=0.01), 4.4° difference in external rotation at 90° abduction (15.6°¹8.5° vs. 20.0°¹11.7°, P=0.007), and 10.6° difference in internal rotation at 90° abduction (10.8°¹9.5° vs. 21.4°¹9.5°, P<0.001) [50]. There was no difference in internal rotation at adduction between the two groups. The decreases in external rotation (3.4° in adduction and 4.4° in 90° of abduction), though statistically significant, may not be of clinical importance [50]. In contrast, the 10.6° difference in internal rotation at 90° of abduction may negatively affect elite athletes who require such movement [50]. Finally, a finite element analysis by Feng et al. [51] in 2022 compared Bankart repair alone with Bankart repair with remplissage, considering the number and positions of the remplissage anchors. They found that a larger number of anchors and medial positioning were associated with greater shoulder stability, but at the cost of decreased ROM [51].
Return to Sports
Arthroscopic Bankart repair with remplissage augmentation has effectively allowed many patients with anterior shoulder instability to RTS, both at any level and at previous level of play. However, the reported RTS rates are not congruent across all types of sport. Therefore, a patientâs specific activities are important to consider when discussing remplissage. A systematic review and meta-analysis by Davis et al. [52] explored the RTS rates, outcomes, and adverse events of arthroscopic Bankart repair with remplissage compared to Bankart repair alone and the Latarjet procedure in 538 patients. The authors reported an overall RTS rate of 86% in patients who underwent arthroscopic Bankart repair with remplissage, with 74% returning to previous level or higher [52]. The RTS rate was stratified by athlete type, as 88% for competitive athletes, 98% for professional athletes, 88% for contact or collision athletes, and 84% for throwing or overhead athletes [52]. The RTS rates for arthroscopic Bankart repair with remplissage were significantly greater than those of Bankart repair alone and of Latarjet. Their findings suggest that addition of remplissage to Bankart repair significantly improves the overall RTS rates [52]. Another systematic review, however, reported overall RTS rates ranging from 60% to 100% in 736 athletes who underwent arthroscopic Bankart repair with remplissage, with 63% to 100% returning to their previous level [53]. While contact or collision athletes had an RTS rate ranging from 80% to 100%, a lower rate was determined for overhead or throwing athletes, 46% to 79% [53].
Complications
In general, the remplissage procedure demonstrates a favorable safety profile and low incidence of complications compared to other procedures. A systematic review by Gouveia et al. [54] compared the outcomes of arthroscopic Bankart repair with remplissage (961 patients) to those of bone block augmentation procedures (6,870 patients). The authors reported complication rates of 0% to 2.3% in patients treated with remplissage, with the only complications being transient neuropraxia (n=1), adhesive capsulitis (n=1), and deep wound infection (n=1) [54]. These complications are contrasted to the higher rates seen in bone block procedures, which range from 0% to 67% and include nonunion, fracture (266/461), infection (65/461), and nerve injuries (45/461) [54]. Another systematic review reported a seven-fold significant increase in the risk of complications in the Latarjet procedures (9%) compared to the remplissage (1%) [40]. One concern with the remplissage procedure, however, is the potential loss of external rotation postoperatively, which has been documented in several studies and described in the previous section [40].
With regard to postoperative stability and recurrence, Davis et al. [52] found that the mean recurrence rate after remplissage was 7.3% and 5.0% for overall patients and athletes, respectively, which was significantly lower compared to patients who underwent Bankart repair alone or Latarjet. Yang et al. [37] found that the following patients who underwent remplissage had a higher risk of recurrence compared to those who underwent Latarjet: collision and contact athletes; patients who had undergone previous instability surgery; patients with 10%â15% preoperative glenoid bone loss; and patients with >15% preoperative glenoid bone loss. Finally, a retrospective study by Paul et al. [55] explored the outcomes of 28 patients who underwent Bankart repair with remplissage and 43 patients who underwent Latarjet at a mean follow-up of 3.3 years. The authors [55] found higher subjective shoulder instability in the remplissage group (50% vs. 21%), although patients who underwent Latarjet had greater bone loss preoperatively than did those in the remplissage group (19% vs 11%). Therefore, while the remplissage procedure has a relatively low recurrence rate, evidence confirming its superiority over other bone block procedures remains equivocal, especially in patients with critical bony defects.
RECOMMENDATIONS
Addition of remplissage to arthroscopic Bankart repair is a great tool for shoulder surgeons addressing anterior glenohumeral instability. The soft-tissue filling procedure has the potential to decrease recurrence rates and improve joint laxity in a manner that is less invasive than the more robust Latarjet procedure. The clinical outcomes following the remplissage have generally been favorable for a majority of patients, and its complication rates are lower than those of more invasive bone blocking procedures. Therefore, patients should be educated about the remplissage and its use as a valid surgical option for anterior instability.
That being said, and like other procedures, the remplissage has its limitations. Several studies have raised concerns regarding its efficacy in patients with significant glenoid bone loss or HSL, especially compared to the Latarjet. In addition, several studies have described limitations in ROM (mainly external rotation) because of the infraspinatus tenodesis, which is conducted to fill the HSL.
It is of pivotal importance to properly educate patients on the advantages and disadvantages of all available treatment options. While losing a few degrees of external rotation may be insignificant to one athlete, it can be detrimental to another athlete whose sport heavily relies on the external rotation needed to throw. Our expert opinion is to avoid using the remplissage in patients with greater than 15% glenoid bone loss, greater than 25% HSL, high risk of recurrence, and in those who engage in overhead throwing activities. Accordingly, the management options should be catered to the individual patient, who should be actively involved in the decision.
CONCLUSIONS
Anterior shoulder instability is a very common complaint in the general population. Several surgical procedures have been proposed to treat patients with different degrees of anterior shoulder instability. One relatively novel procedure is the remplissage, which is conducted in conjunction with arthroscopic Bankart repair, to treat off-track HSLs. The remplissage has gained worldwide popularity as a minimally invasive technique that improves shoulder stability. In addition, its outcomes are generally comparable to those of more invasive bone-blocking procedures, and it has a relatively low risk profile. Nevertheless, there are concerns about its efficacy in more critically unstable patients and the ROM limitations that often arise after this procedure. As with most surgical procedures, a patient ought to be educated about the advantages and disadvantages and be actively involved in the management discussion. Regardless, the remplissage remains a valuable procedure with great potential in providing benefit to patients with shoulder instability. Additional comparative studies and multicenter clinical trials should be conducted to further confirm the utility of this procedure and establish its place in the current treatment guidelines.