INTRODUCTION
Partial distal biceps tendon (DBT) tears are a unique clinical entity. Patients often present sub-acutely, and signs and symptoms may be subtle or non-specific [1,2]. Recent study has identified morphological differences between elbows with partial DBT tears compared to non-diseased controls, including a higher frequency of bifid tendons and a narrower radio-ulnar space [3].
In complete DBT tears, operative fixation is generally recommended. Anatomic repairs have become standard and can be achieved using intraosseous Endobuttons, transosseous reinsertion suture anchors, interference screws, or transosseous sutures [4-6]. Conversely, in partial DBT tears, optimal management remains contentious. There is a paucity of literature on the characteristics of different tears and on repair techniques for partial tears, and it is unclear whether partial tear disruption affects more or less than 50% of the DBT insertion [7-9].
A short head and a long head make up the biceps musculotendinous unit. The long head arises from the superior aspect of the glenoid and the short head from the coracoid process. These two muscle bellies remain separate, and most tendons are discrete entities at the musculotendinous junction [10-13]. Multiple studies have investigated the anatomy of the DBT as it inserts onto the radial tuberosity [10,12-15]. With increased understanding of the insertional anatomy of the DBT, we have begun to appreciate the separate roles of the long head and short head [13,16,17].
Recent studies have identified DBT anatomy using high-resolution 3-tesla magnetic resonance imaging (3T MRI) [3,11]. 3T MRI imaging has a higher signal-to-noise ratio than 1.5-T images, which allows better anatomic resolution [18] making it well suited for characterizing precise in vivo anatomy. Given the paucity of data on different types of partial DBT tears, the purpose of this study was to define the pathoanatomy of the partially torn DBT using 3T MRI and to develop a classification system for this heterogeneous group.ŌĆā
METHODS
Institutional review board approval was received for this study from the Health and Disability Ethics Committee, New Zealand (Ref. 21/CEN/187). Informed consent was waived due to retrospective nature of this study.
All MRI scans performed over a 2-year period at our institution on elbows for any indication were screened, and all partial tears were noted for closer review. A total of 44 dedicated 3T MRI scans of elbows with partial DBT tears from our institutionŌĆÖs Picture Archiving and Communication System imaging system retrospectively was reviewed. These were obtained from patients undergoing treatment for partial DBT tears for elbow pain persisting at least 6 weeks post injury. Exclusion criteria included skeletally immature patients, motion artefact/poor quality scans, and incomplete/inappropriate scans. All scans were performed using the Siemens Vida 3T with slice thickness set to 3 mm. All scans were performed using the institutionŌĆÖs standard protocol with the elbow extended and the upper limb next to the trunk to allow true axial and sagittal slices. Sequences reviewed were either sagittal PD TSE (FOV 140├Ś140) and axial PDFS TSE (FOV 100├Ś100) (Figs. 1-4) or sagittal PDFS TSE (FOV 140├Ś140) and axial PDFS (FOV 100├Ś100) (Fig. 5). Basic demographic data including age, sex, and side (right or left) were collected. Mechanism of tear was also noted from the patientŌĆÖs electronic record.
Measurements
Each scan was reviewed independently by two trained observers: a fellowship-trained upper limb surgeon (SBMM) and an orthopaedic surgeon (ABB) in training. Each scan was reviewed for the presence or absence of retraction of the torn part of the tendon and the presence of discrete long-head and short-head tendons at the DBT insertion (a ŌĆ£bifidŌĆØ tendon), and tear morphology was noted to document the percentage of insertion involved and the anatomic position of the tear.
Retraction
The presence or absence of retraction of the torn part of the tendon, defined as visible retraction >5 mm, was noted for each patient. This was reviewed by analysing the sagittal images using the axial plane for clarity and by measuring from the radial tuberosity to visible torn tendon edge.
Bifid Tendons
The presence of discrete long-head and short-head tendons at the DBT insertion (a bifid tendon) was also noted. Images were reviewed at the musculotendinous junction in both the sagittal and axial planes to see if two discrete tendons or a single tendon was visible. In cases where two discrete tendons were visible at the musculotendinous junction, images were traced along the axial plane to see if the tendons interdigitated at some point or whether they continued to their insertion/the tear as two discrete tendons (a bifid tendon).
Enthesophytes
Enthesophytes were defined as bony proliferations oriented along the line of the tendon fibres at the insertion point of the DBT at the radial tuberosity. The axial and coronal planes were used to assess the presence of enthesophytes as determined by independent observers.
Tear Morphology
Each scan was carefully reviewed by the two observers (ABB and SBMM) in both the axial and sagittal planes. Once the tear was identified, tear morphology was recorded by measuring the approximate percentage of the footprint involved (i.e., tear length divided by total insertion length) as well as the part of the insertion that was torn (i.e., distal, proximal, radial, ulnar, or a combination). The written descriptions of tear morphology were retrospectively reviewed by the two observers to identify recurring tear types.ŌĆā
RESULTS
The mean age of the 44 participants was 52 years (range, 34ŌĆō72 years). There were 36 males and 8 females. All patients described a traumatic mechanism: 37 with eccentric loading/lifting/wrenching injuries, 6 with traumatic hyperextension injuries, and 1 with concentric loading with supination.
Retraction
Retraction was seen in 5 of 44 partial tears (11%). Of these 5 tears with retraction, 1 was a long-head only tear and the other 4 were short-head only tears.
Bifid Tendons
At their insertion onto the radial tuberosity, 13 of the 44 DBTs were bifid tendons (30%).
Tear Morphology
All tears fit into one of five categories. The relative frequencies and descriptions of each tear type are outlined in Table 1. The descriptive data on tear morphology were consistent between observers for all scans.
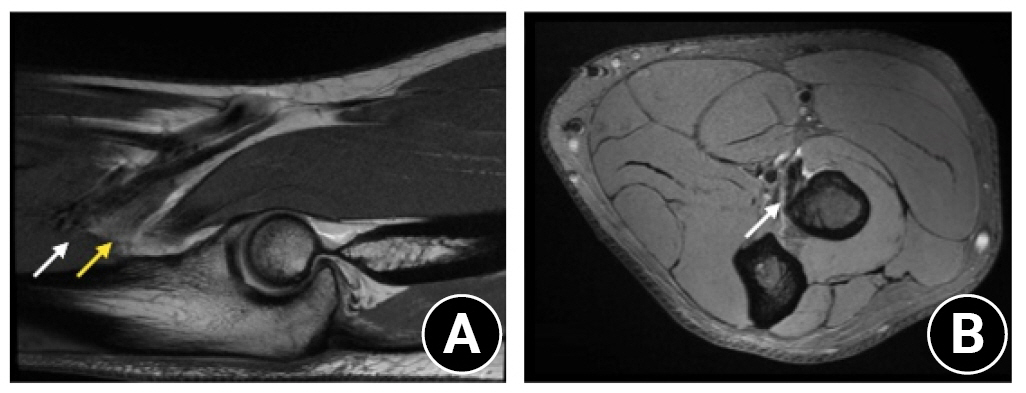
Group 1 consisted of single tendons in which only the most proximal up to 50% of the insertion was involved or bifid tendons in which there was an isolated tear of the proximal head with no tear/involvement of the distal head. These were considered long-head only tears (Fig. 1).
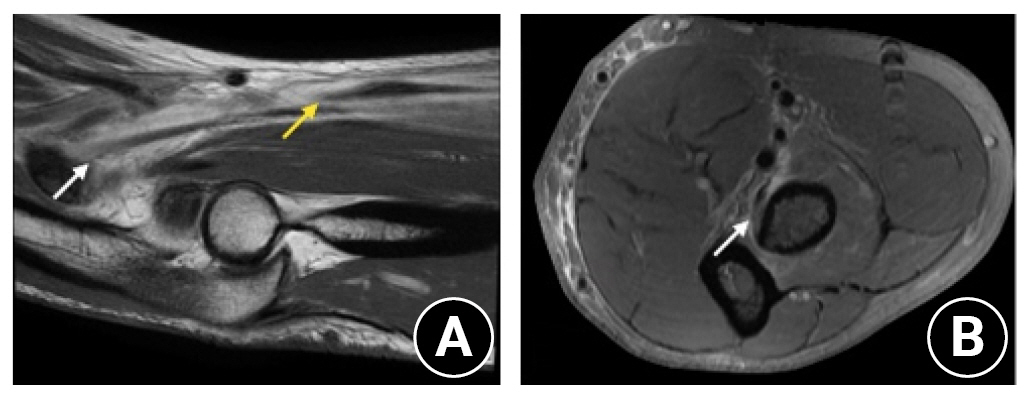
Group 2 consisted of single tendons in which only the most distal up to 50% of the insertion was involved or bifid tendons in which there was an isolated tear of the distal head with no tear/involvement of the proximal head. These were considered short-head only tears (Fig. 2).
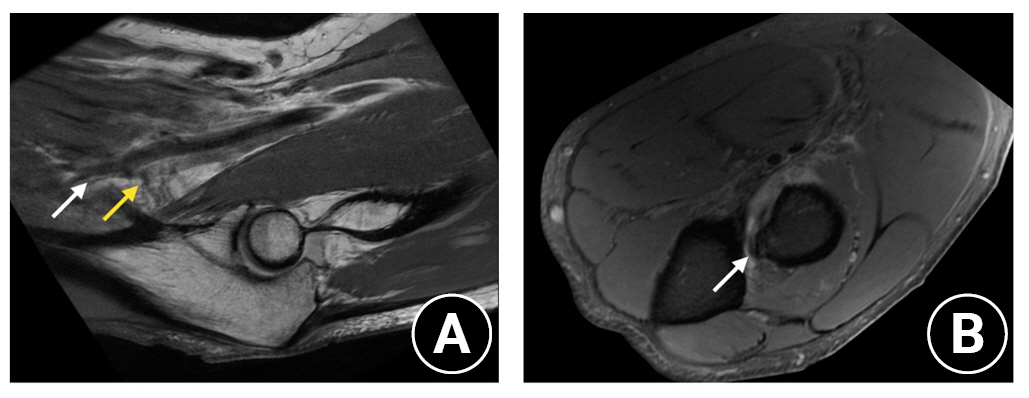
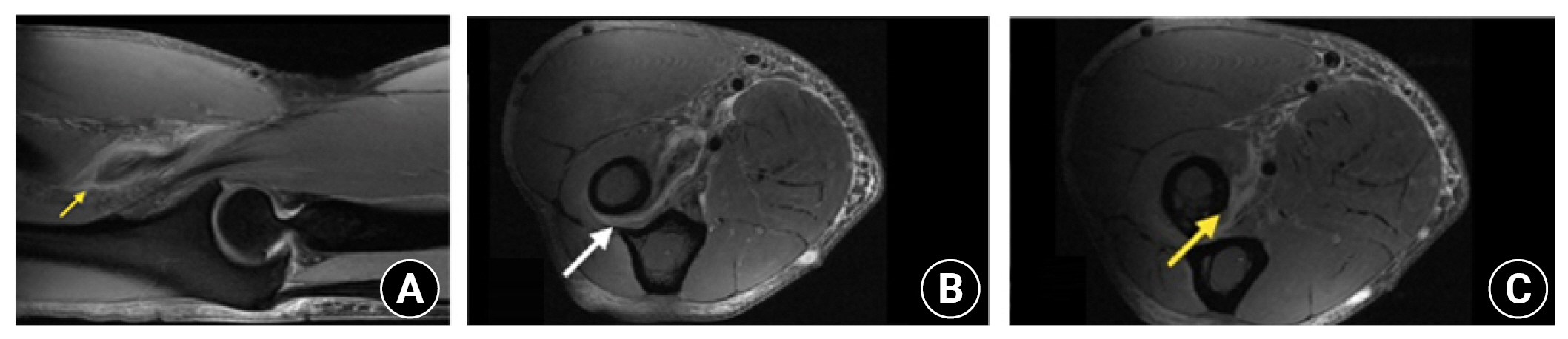
Group 3 consisted of single tendons in which the most proximal up to 50% of the insertion was involved as well as further extension of the tear into the distal insertion or bifid tendons in which there was a complete tear of the proximal head with a partial tear/some involvement of the distal head. These were considered complete long head with partial short-head tears (Fig. 3).
Group 4 consisted of single tendons in which the most distal up to 50% of the insertion was involved as well as further extension of the tear into the proximal insertion or bifid tendons in which there was a complete tear of the distal head with a partial tear/some involvement of the proximal head. These were considered complete short head with partial long-head tears (Fig. 5).
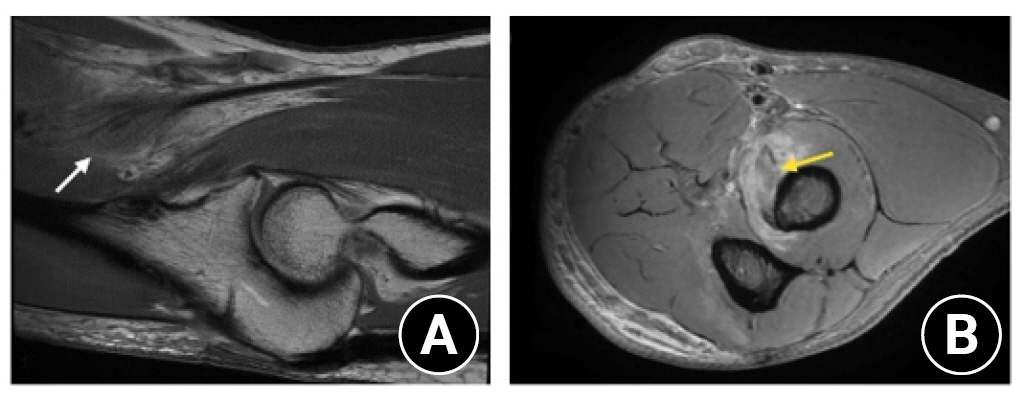
Group 5 consisted of tendons in which there was oedema and partial lift-off at the insertion at any point but no clear involvement of the entire proximal or distal insertion. These were considered peel-off tears (Fig. 4).
DISCUSSION
Our results reveal five main types of DBT partial tears identified on 3T MRI scan: long head isolated tears, short-head isolated tears, complete long-head tears with partial short -head involvement, complete short-head tears with partial long-head involvement, and peel-off tears. Understanding these tear types requires good understanding of the anatomy of the DBT.
The biceps musculotendinous unit consists of the long head and the short head. The long head arises from the supraglenoid tubercle and the short head from the coracoid process. The two corresponding muscle bellies remain separate, and most DBTs have discrete long-head and short-head tendons at the musculotendinous junction [10-13]. The long-head and short-head parts of the DBT may remain discrete or interdigitate to varying degrees as the DBT runs to its insertion on the radial tuberosity [10-13] during which time it rotates and the orientation of the two heads changes. The short head becomes superficial and the long head becomes deeper and sits slightly more laterally [10,19,20]. The DBT then inserts onto the radial tuberosity. The long head part of the DBT inserts more proximally on the radial tuberosity, while the short-head part inserts further distally [10,12,13,20]. Several cadaveric studies have supported these unique insertions of the two heads of the DBT onto the radial tuberosity [10,12,13,20]. However, a study by Bhatia et al. [14] did note large variations in footprint insertions.
The pathogenesis of partial DBT tears is relevant to understanding their differing morphologies. A large radial tuberosity or a narrow radio-ulnar space may impinge on the DBT, leading to chronic change and attritional rupture with time. This theory is supported by the finding that the space through which the DBT runs between the lateral ulna and radial tuberosity may decrease as much as 50% from supination to pronation even in non-diseased elbows [21-23]. In a comparative control MRI study of 26 normal elbows and 26 partial tears, significantly larger measurements for radial tuberosity length, radial tuberosity thickness, and ratio of radial tuberosity thickness to radial diameter were found, as well as a statistically significant smaller radio-ulnar space [3]. A significant association also was found between partial tears and enthesophytes, likely for the same reason [3]. In the same study, two discrete tendons was significantly more common in the partial tear group [3]. In the present study, 13 of the 44 DBTs were bifid tendons at their insertion onto the radial tuberosity (31%). It is possible that a discrete tendon predisposes one to particular partial tears. More research is needed in this regard.
There is conflicting evidence on the frequency of complete discrete short-head and long-head DBTs (as opposed to a single DBT tendon or, more commonly, two discrete tendons that interdigitate prior to insertion). Three cadaveric studies, all including 15 to 25 cadavers, have shown differing results. Cho et al. [12] found that 48% of DBTs consisted of two distinct and easily separated parts, while 52% interdigitated completely into a single distal tendon. Eames et al. [13] found that 59% of DBTs consisted of two distinct tendons, while 41% interdigitated prior to insertion. Athwal et al. [10] found that 13% of DBTs consisted of two separate tendons, 54% were attached but easily separable, and 33% were inseparably interdigitated. An MRI study of 106 DBTs found that 82% of tendons interdigitated prior to insertion onto the radial tuberosity, while 8% remained as two visibly discrete tendons for their entire length, remaining as two discrete insertions at their origin at the musculotendinous junction and remaining separate until their two adjacent but separate insertions at the radial tuberosity [11]. The independence of the two tendons has implications for classification and management.
The surgical management of complete DBT tears has been reported in the literature. For partial DBT tears the evidence is less clear; to our knowledge there is no literature to suggest which surgical intervention is most appropriate for any particular partial tear. Surgical intervention clearly has its place, although Bauer et al. [24] demonstrated that high-need patients with partial DBT tears reported better recovery post-surgery than with conservative management, and that 55.7% of partial DBT patients initially managed conservatively eventually underwent surgery. Previous studies characterizing partial DBT tears using MRI have divided partial tears into high-grade partial tears requiring surgical intervention (tendonous disruption affecting more than 50% of the DBT insertion) and low-grade partial tears not requiring surgical intervention (tendonous disruption affecting less than or equal to 50% of the DBT insertion) [7-9]. The utility of this number (50%) as a guide for surgical management is unclear, although a significant decrease of supination strength has been reported when the tear involves more than 75% of the footprint [25]. Operatively managed partial tears are often treated by surgically transecting the remaining intact DBT and performing a complete anatomic repair using the methods outlined above [26,27]. This has similar outcomes to the treatment of complete DBT ruptures [1] but may lead to overly aggressive treatment of some tears. Endoscopic techniques allow intra-operative assessment of tears that may not require full complete release and reinsertion [2].
The anatomy of the insertion may have biomechanical implications relevant to surgical management. If the long head of the DBT inserts more proximally and the short head more distally, [10-13] this may position the short-head DBT to be a more powerful flexor and the long head DBT as a more powerful supinator, as has been reported in previous biomechanical studies [13,16,17]. The proposed mechanism for this involves the moment arm of each head. When the arm is in a neutral or pronated position the moment arm for the short head (the length between the elbow joint axis and the line of force acting on the joint) is larger given its more distal insertion. This makes it a more powerful flexor. Likewise, the more proximal long head insertion is further from the axis of rotation of the forearm, making it a more powerful supinator [13,16,17].
Given the reliance on biceps brachii for supination, perhaps we should be more proactive in fixing long-head only tears. If the long head is the primary supinator, isolated long head ruptures may be best managed with detachment and surgical repair of the single head. Conversely, if the short head is the primary flexor, isolated short-head tears may be appropriate to scope/debride in low demand patients and only proceed to detachment and repair in high demand patients, given that brachialis functions well as a flexor.
By this logic, complete detachment and anatomic repair might be appropriate in complete long head tears with partial short-head involvement and complete short-head tears with partial long head involvement. The peel-off lesions noted in this study bear a significant resemblance to partial articular supraspinatus tendon avulsion (PASTA) lesions. These might be best managed in a similar fashion to an arthroscopic PASTA repair by endoscopically reviewing the tendinous insertion, maintaining any healthy fibers on the footprint, and repairing those that are peeling off.
These proposed management plans are simply hypotheses regarding the different tear types noted in this study. The management outlined above relies heavily on the biomechanical studies that state the short-head DBT is positioned to be a more powerful flexor, and the long head DBT to be a more powerful supinator [13,16,17]. A biomechanical study by Tomizuka et al. [25] contradicted these findings; however, showing that a simulated short-head avulsion significantly decreased the supination strength. Clearly, further biomechanical studies are required to determine the contribution of each component of the DBT to specific biceps function, and our MRI based classification needs to be verified by surgical or cadaveric studies.
This study had several limitations. First, this was an MRI study with no surgical correlation. Although MRI is the radiological gold standard for characterizing DBT injuries, it has been reported that there is not always correlation with surgical findings in partial DBT tears, albeit using 1.5T MRI, rather than 3T MRI [20]. MRI is also expensive and not necessarily readily available for all patients, and this may reduce the generalizability of the findings. Ultrasound has, in one case, shown the potential to differentiate between isolated lesions of the short head or long head [20]. Second, although it is possible to trace the short-head and long-head components of the DBT from musculotendinous junction downwards, in injured tendons the anatomy can be distorted. Our interpretation of each tear (and therefore our classification system) relies in part on the known anatomy of the DBT tendon (which may be unknowingly erroneous) rather than direct visualisation. Third, the sample size in the current study was small, meaning our descriptive study and classification system may not capture the full diversity of partial DBT tears and does not provide a solid basis for epidemiological insight. Nevertheless, this is foundational knowledge on which to build upon and represents the first proposal for a partial DBT tear classification system which may have implications for management looking forward. Future research should consider larger sample sizes, explore correlations with surgical findings, compare the effectiveness of more accessible imaging modalities, and identify the clinical implications of different tear types. Further prospective studies are required to assess an algorithm for treatment of these partial DBT tears.
CONCLUSIONS
Using 3T MRI scans have investigated the tear morphology of partial DBT tears and have proposed a classification system for these injuries. This descriptive study and classification system will allow further investigation into partial DBT tears and will promote further investigation into the management of these heterogeneous injuries.