Use of custom glenoid components for reverse total shoulder arthroplasty
Article information

Abstract
Background
Our purpose was to evaluate a custom reverse total shoulder arthroplasty glenoid baseplate for severe glenoid deficiency, emphasizing the challenges with this approach, including short-term clinical and radiographic outcomes and complications.
Methods
This was a single-institution, retrospective series of 29 patients between January 2017 and December 2022 for whom a custom glenoid component was created for extensive glenoid bone loss. Patients were evaluated preoperatively and at intervals for up to 5 years. All received preoperative physical examinations, plain radiographs, and computed tomography (CT). Intra- and postoperative complications are reported.
Results
Of 29 patients, delays resulted in only undergoing surgery, and in three of those, the implant did not match the glenoid. For those three, the time from CT scan to implantation averaged 7.6 months (range, 6.1–10.7 months), compared with 5.5 months (range, 2–8.6 months) for those whose implants fit. In patients with at least 2-year follow-up (n=9), no failures occurred. Significant improvements were observed in all patient-reported outcome measures in those nine patients (American Shoulder and Elbow Score, P<0.01; Simple Shoulder Test, P=0.02; Single Assessment Numeric Evaluation, P<0.01; Western Ontario Osteoarthritis of the Shoulder Index, P<0.01). Range of motion improved for forward flexion and abduction (P=0.03 for both) and internal rotation up the back (P=0.02). Pain and satisfaction also improved (P<0.01 for both).
Conclusions
Prolonged time (>6 months) from CT scan to device implantation resulted in bone loss that rendered the implants unusable. Satisfactory short-term radiographic and clinical follow-up can be achieved with a well-fitting device.
Level of evidence
III.
INTRODUCTION
Glenoid bone loss, primary or due to failed arthroplasty, is a problem encountered during reverse total shoulder arthroplasty (RTSA) procedures [1,2]. Management of glenoid bone loss in these situations is challenging, particularly when eccentric glenoid wear is present. Bone grafting for such defects has been reported for primary shoulder arthroplasty, as well as after bone loss from infection, glenoid component failure in anatomic shoulder arthroplasty, and revision of a failed RTSA [1-4]. However, bone grafting for large glenoid defects has been reported to have a high failure rate when used for those indications because the bone stock might not be adequate for conventional implants to gain adequate purchase [4].
Recently, the use of custom glenoid components has been shown to provide short-term success in treating large glenoid bone defects [5-8]. These components are manufactured to fill a bone defect with a metallic glenoid component that includes a baseplate that mirrors the bone surface and provides bone fixation with multiple screws. Several previous studies have reported short-term success with custom glenoid components in RTSA, but those studies have typically involved multiple surgeons, and only one of them reported any intraoperative or postoperative complications (Table 1) [5-9].

Previous publications about the use of custom glenoid implants
Our goals in this study were to report the preoperative assessment of patients undergoing RTSA with a custom glenoid component, describe intraoperative complications associated with the use of these devices, and report the short-term clinical and radiographic results and complications from using custom glenoid components.
METHODS
This study was approved by the Institutional Review Board of Johns Hopkins Medicine (No. 00279172). The requirement for informed consent was waived.
We used our institutional shoulder arthroplasty registry to identify patients who underwent shoulder replacement with a custom glenoid prosthesis between January 2017 and September 2022. The inclusion criterion was loss of glenoid bone to the extent that computer modeling predicted inadequate bone coverage of the glenoid baseplate when using conventional or augmented baseplates—this process is performed for all preoperative patients undergoing RTSA. Inadequate bone was defined as coverage of less than 50% of the baseplate on computer modeling [9].
During this period, 1303 RTSAs were performed by the senior author (EGM); of them, 29 (2.2%) were eligible for custom glenoid vault components (Fig. 1). The glenoid vault deformities were classified using the criteria of Walch [10,11], Antuna [12], Hamada [13], Sirveaux [14], and Frankle [15]. Of the 29 eligible patients, COVID pandemic-related delays made four ineligible for surgery for medical reasons, and one of those four patients died. That left 25 patients who underwent reconstruction using a custom glenoid vault designed for their individual glenoid morphologies (Comprehensive Vault Reconstruction System, Zimmer Biomet). At the time of surgery, three implants did not fit the glenoid, and as a last resort, all of those patients received standard manufactured baseplates and available RTSA components from a different implant system (ReUnion RSA; Stryker) despite less-than-optimal glenoid coverage by the baseplate. Median follow-up was 18 months (range, 1–60 months) in the remaining 22 patients, nine of whom had >2 years of follow-up (range, 24–60 months) (Fig. 2).

Example patient who previously sustained an anatomic total shoulder arthroplasty and underwent antibiotic spacer placement for prosthetic joint infection. Preoperative radiographs (A-C) show the antibiotic spacer and severe glenoid bone loss. Computed tomography scan images (D-F) highlight the severity of bone loss due to osteolysis and previous glenoid screws.
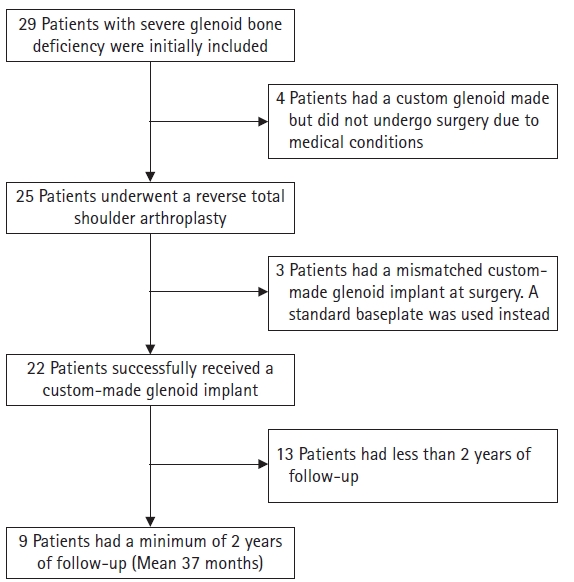
Flow diagram for the 29 cases of custom glenoid replacement for significant glenoid bone loss.
All patients underwent a preoperative assessment (plain radiographs, computed tomography (CT) scans, and a thorough physical examination) within 1 month of surgery (Fig. 3). All patients deemed to require a custom glenoid component received thin-cut CT scans in line with a protocol that enables three-dimensional (3D) modeling. All patients underwent computer modeling of the glenoid by engineers from the company to determine the trajectory and length for each screw that provided the best orientation to reach the most substantial bone [8]. This analysis was performed for the central non-locking screw and four peripheral locking screws.
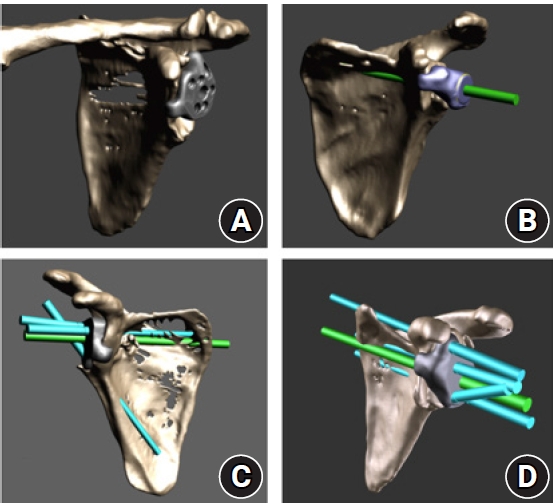
(A-D) Three-dimensional modeling demonstrating the planned position for the custom glenoid component and the central screw (green) and peripheral locking screw (blue) trajectories.
Visual analog scale (VAS) scores for pain and several patient-reported outcome measures (PROMs) were collected from each patient: the shoulder score from the American Shoulder and Elbow Score (ASES) [16], the Simple Shoulder Test (SST) [17], the Single Assessment Numeric Evaluation (SANE) [18], and the Western Ontario Osteoarthritis of the Shoulder Index (WOOS) [19]. The minimal clinically important differences (MCIDs) for the PROMs and ranges of motion (ROMs) [20] were used to determine clinically meaningful improvement after surgery. Preoperative clinical outcome scores were gathered within 1 month preoperatively and at 3 months, 6 months, 1 year, and then annually postoperatively.
The preoperative and postoperative physical examinations were performed by one of two observers (the senior author [EGM] or senior author’s physician assistant, who had 12 years of experience) to minimize inter-observer variability [21]. The examination included ROM; strength testing in abduction; external rotation with the arm at the side; and lag signs, particularly the external rotation lag sign [22], the dropping sign [23,24], and the lift-off lag sign [25]. Plain radiographs were taken from an anterior-posterior view in internal rotation, a true anterior-posterior view (Grashey view) [26], and an axillary view. The mean interval from the CT scan to the day of surgery for patients who successfully received a custom glenoid implant was 5.7 months (range, 1–10.7 months). For patients who had a custom glenoid made that did not fit intraoperatively, the mean duration was 7.8 months (range, 5.9–10.7 months). Three-dimensional imaging and physical models were made available during the preoperative and intraoperative periods to assist in planning implant orientation, screw trajectory, and optimal fixation. Postoperatively, the patients underwent only plain radiography at each subsequent office visit. All radiographs were read by independent observers for implant movement, loosening of the baseplate or screws, and scapular notching.
Operative Technique
After an administration of antibiotics and the induction of general anesthesia, all patients were placed in the beach-chair position. A deltopectoral approach was used to develop an interval down to the clavipectoral fascia. After arthrotomy was performed, the proximal humerus was exposed, and a freehand transverse cut was made with an oscillating saw in approximately 30° of retroversion and 135° of inclination after marking the planned cut with a cutting guide. The glenoid was then carefully and thoroughly exposed such that the entire glenoid rim and vault could be completely visualized using a posterior-inferior Hohman retractor, posterior glenoid access retractor, and superior Hohman retractor. The glenoid defect was then compared to the scapular model, and the glenoid component was placed in the glenoid using the handle. If the implant could not be fitted exactly to the surface of the glenoid, it was deemed to toggle, which was interpreted to mean that the interface between the component and the glenoid surface was inexact due to either excess bone or soft tissue interposition. A 6.5-mm central screw was then placed in the central hole and inserted. In several instances, the screw did not provide compression. In such cases, the screw was deemed a spinner, meaning that it provided no compression and did not have firm fixation. Peripheral locking 4.75-mm screws were then placed according to the depth-guide-measured depth.
In the three patients whose implants did not fit the glenoid at all, the glenoid was reamed to a flat surface, and a different implant system (Stryker ReUnion Stryker) with a central screw and two peripheral screws was used as a last resort. In all three of those cases, less than 50% of the glenoid bone remained, but a hemiarthroplasty was not performed out of concern about subsequent instability of the prosthesis.
Outcomes and Data Analysis
The demographic and clinical findings are summarized with descriptive statistics. Preoperative clinical outcomes (SST, ASES, WOOS, VAS), ROM values, and patient satisfaction were compared with the patient’s most recent postoperative visit using the Wilcoxson signed-rank test. Radiographs were evaluated by two fellowship-trained shoulder surgeons for any signs of loosening, osteolysis, or subsidence. To determine differences in treatment outcomes, a subgroup analysis between primary and revision cases was conducted using the Mann-Whitney U-test.
RESULTS
The mean time from the index CT scan to the day of surgery (regardless of whether a custom glenoid was ultimately placed) was 5.7 months (range, 1–10.7 months). For patients who had a custom glenoid made that did not fit intraoperatively, the mean duration was 7.8 months, whereas those who received a custom glenoid had a mean duration of 4.8 months. The mean follow-up was 2.8±0.5 years.
Intraoperative fracture occurred in seven cases (31.8%), including one of the scapular spine (4.5%), one of the medial calcar of the proximal humerus (4.5%), five of the greater tuberosity (22.7%), and one of the greater tuberosity with a simultaneous fracture of the proximal humeral shaft (4.5%). The central screw was deemed a spinner in eight cases (36.4%), and an unexpected positive culture (Cutibacterium acnes) was found in six (27.2%). Two other complications, implant toggling and completely missed screw trajectory, occurred in four (18.1%) and two cases (9.1%), respectively. At final follow-up, none of the patients in the study had suffered baseplate failure or dislocation necessitating reoperation.
Of the 22 patients who had a custom glenoid component implanted, the baseplate toggled at the time of surgery in four (18%). In two patients (9%), one peripheral screw did not contact bone, and one screw contacted the cortical bone and was therefore left in place. In a third patient, the screw had no contact with bone and as a result was not used. The nine patients (5 primary, 4 revision) who had a minimum 2 years of follow-up were five females and four males (mean age, 74.3±5.3 years; body mass index, 28.2±5.5 kg/m2). The etiologies in the five primary cases were degenerative arthritis in one, cuff tear arthropathy in two, and posttraumatic arthritis in two. The four patients who underwent revision had each had at least two prior arthroplasty surgeries (Table 2).

Characteristics of nine patients with minimum 2-year follow-up after RTSA
Table 3 compares the ROMs, clinical outcomes, pain, and satisfaction before and after the RTSA with a custom implant. Significant improvements were observed in all PROMs in the nine patients with a minimum of 2 years of follow-up (ASES, P<0.01; SST, P=0.02; SANE, P<0.01; WOOS, P<0.01). ROM improved significantly for forward flexion and abduction (P=0.03 for both) and internal rotation up the back (P=0.02). Pain and satisfaction were also significantly improved (P<0.01 for both) (Table 3).

Ranges of motion, clinical outcomes, and pain before and after RTSA with custom implant in nine patients with minimum 2 years of follow-up
DISCUSSION
Our results show that a custom glenoid implant is a viable option for severe glenoid bone loss in both primary and revision RTSA. However, our results also demonstrate that these implants should be implanted within a few months of construction, that imperfect fit of the implant can occur, and that complications typical of cases with complex glenoid bone loss can occur. Nonetheless, custom glenoid components used for RTSA can, at early follow-up, provide statistically and clinically significant Preoperative to postoperative improvements in pain relief, PROMs, ROM, and patient satisfaction, with patients experiencing improvement in pain and functional outcomes that met the criteria for MCID [20]. This study also highlights special considerations in Preoperative planning, intraoperative positioning of the implant, and postoperative follow-up for these patients.
Keeping the time from the index CT scan used for modeling and manufacturing the custom glenoid prosthesis to the time of implantation in the patient to a minimum is important. Indeed, the manufacturer suggests that this time be as short as possible because the glenoid bone topography can change if the interval from the CT scan to insertion is too long [27]. In this study, the mean interval in cases with severe mismatch was 7.8 months (range 5.9–10.7 months). Rangarajan et al. [8] noted that manufacture of these devices typically takes a minimum of 8 weeks, and subtle changes in glenoid bone morphology can occur even during that short period. When the custom glenoid component interfaced well with native bone, we found the fit to be nearly perfect, which can rarely be obtained with off-the shelf glenoid components in patients with severe glenoid bone loss. We are not aware of published literature that compares the manufacturing time for custom glenoid implants between implant companies; however, that could be an important topic for future studies.
Our results also highlight the importance of telling patients that the implant might not fit and having a surgical backup plan should the implant not fit at all. In our study, eccentric reaming of the glenoid was performed to the best of our ability in three cases with >50% glenoid bone loss when the custom glenoid implant did not fit adequately. Although none of our patients required revision surgery within the current follow-up period, longer follow-up is needed to determine whether the three patients whose custom implants did not fit have durable long-term results. Another option in these circumstances would be to place a hemiarthroplasty with no glenoid component, but the inability of the custom implant to fit reinforces the importance of having a backup system available for all the possible options in this situation.
This study is the first to present RTSA cases using a custom baseplate with a minimum 2 years of follow-up. Dines et al. [7] reported two patients with failed previous shoulder arthroplasty who were treated with patient-specific implants using a vault reconstruction system. At 18 months’ follow-up, those patients had increased ROM and satisfaction with the surgery. In their multicenter report of experience using a custom glenoid for treatment of severe glenoid deficiency, Debeer et al. [6] found that patients reported high satisfaction, low pain, and good functional outcomes postoperatively. Bodendorfer et al. [5] reported short-term outcomes of custom glenoid placement in 12 shoulders of 11 patients. At a mean follow-up of 30 months, the patients had no complications or any signs of implant loosening. Rangarajan et al. [8] reported on 18 patients with a minimum 1 year of follow-up (mean, 18.2 months). They also reported no failures, with no signs of notching, humeral or baseplate loosening, or implant failure.
The complications seen in this study are comparable to those reported in the literature for custom glenoid components and revision shoulder arthroplasty, with the relatively high rate of complications reflecting the challenging nature of complex revision surgeries [8]. Complications such as greater tuberosity fracture in both primary and revision cases were recently reported by Wixted et al. [28] and Dolci et al. [29]. Our complications when using a custom glenoid component are similar to those reported by Rangarajan et al. [8], who reported four complications (21%): one greater tuberosity fracture; one humeral perforation requiring a fibular strut graft; one hematoma requiring removal and replacement of the humeral component; and one infection, with removal of the implants and placement of an antibiotic spacer.
Several limitations need to be considered when interpreting the results of this study or considering performing this procedure. First, although the follow-up is the longest reported to date for this type of glenoid implant, the number of patients with at least 2 years of follow-up is small, and the results here might represent a type II error. Second, the mass of metal in these implants and irregular surfaces make it difficult to detect the degree of contact between the implant and the glenoid surface. Our experience with toggling of the implant at the time of surgery, with two patients in whom one of the four peripheral screws missed the glenoid bone entirely and a lack of compression of the central screw in eight patients, suggests that the fit of the implants can be less than ideal.
CONCLUSIONS
The short-term outcomes indicate that RTSA with a custom glenoid baseplate gave patients excellent pain relief and functional outcomes after a minimum of 2 years of follow-up. Although custom glenoid components show promise for the treatment of substantial glenoid bone loss, they are not without challenges. This study showed that a prolonged time (more than 6 months) between CT scanning and device implantation resulted in bone loss that rendered the implants unusable. However, when the device does fit the glenoid, satisfactory short-term results can be achieved.
Notes
Author contributions
Conceptualization: PA, PM, ABH, JB, PL, RM, MJB. Data curation: PM, ABH, JB, PL, RM, MJB. Formal analysis: PA, ABH, JB, PL, EGM. Funding acquisition: EGM. Investigation: PA, MJB, EGM. Methodology: PA, PM, ABH, JB, PL, RM, MJB. Project administration: RM. Resources: PM, ABH, JB, PL. Supervision: PM, ABH, PL, MJB. Validation: PM, PL, MJB, EGM. Visualization: EGM. Writing – original draft: PA, PM, ABH, JB, PL, RM, MJB, EGM. Writing – review & editing: PA, PM, ABH, JB, PL, RM, MJB, EGM.
Conflict of interest
EGM is a consultant for Stryker Corporation, outside of this work. All authors declare that they, their immediate family, and any research foundation with which they are affiliated received no financial payments or other benefits from any commercial entity related to the subject of this article.
Funding
The authors disclose receipt of the following financial or material support for the research, authorship, and/or publication of this article: The Donna and William Marriott Research Fund. This funding source had no role in the design, execution, analyses, interpretation of the data, or decision to submit results.
Data availability
Contact the corresponding author for data availability.
Acknowledgments
For editorial assistance, we thank Denise Di Salvo, MS, and Rachel Walden, MS, in the Editorial Services group of the Johns Hopkins Department of Orthopedic Surgery. We also thank the senior author's physician assistant, Marcy Beard, PA-C, Johns Hopkins Medicine, for her involvement in patient examinations.