INTRODUCTION
Olecranon fractures in elderly patients can present unique challenges for orthopedic surgeons [1,2]. Nonoperative treatment may be appropriate in carefully selected patients with stable fracture patterns; however, functional outcomes are often modest and may result in compromised independence and functional status [1]. Alternatively, operative intervention has been associated with high rates of reoperation and complications in up to 80% of elderly patients with displaced olecranon fractures [3-7].
Complications in elderly patients typically result from hardware failure secondary to poor fixation in significantly osteoporotic bone. This can lead to fracture displacement, wound complications, and infection requiring subsequent reoperation. Advances in locking plate technology have improved outcomes compared with tension-band techniques, but adequate fixation in small osteoporotic bone fragments remains challenging [8,9].
Additionally, wound dehiscence and symptomatic hardware necessitating additional intervention are not uncommon in elderly patients with olecranon fractures treated with a plate [10]. An alternative form of olecranon fracture fixation was described by Bateman et al. [11], which involved transosseous fracture repair with suture anchors. This technique was specifically designed to be utilized with small fracture fragments and, in elderly patients with osteoporotic bone, to mitigate the risk of hardware prominence and fixation failure. No intraoperative complications or reoperations were reported in their initial series of six patients at a mean follow-up of 5 years [11].
We sought to provide an updated clinical series, with a larger population size, younger mean age, and longer follow-up of use of suture anchor fixation in elderly patients with displaced olecranon fractures, and we evaluated the expanding role for this technique in younger patients with small fracture fragments.
METHODS
This study was approved by Institutional Board of Thomas Jefferson University (No. #20E.370). Informed consent was waived for retrospective chart review of the patients but obtained prior to collection of prospective outcomes via questionnaire administration. A retrospective review was performed for all consecutive patients with displaced olecranon fractures treated with suture anchor fixation at a single institution and with at least 2 years of clinical follow-up. Seventeen consecutive patients with Mayo IIa or IIb olecranon fractures were treated with this technique between January 1, 2006, and November 1, 2018.
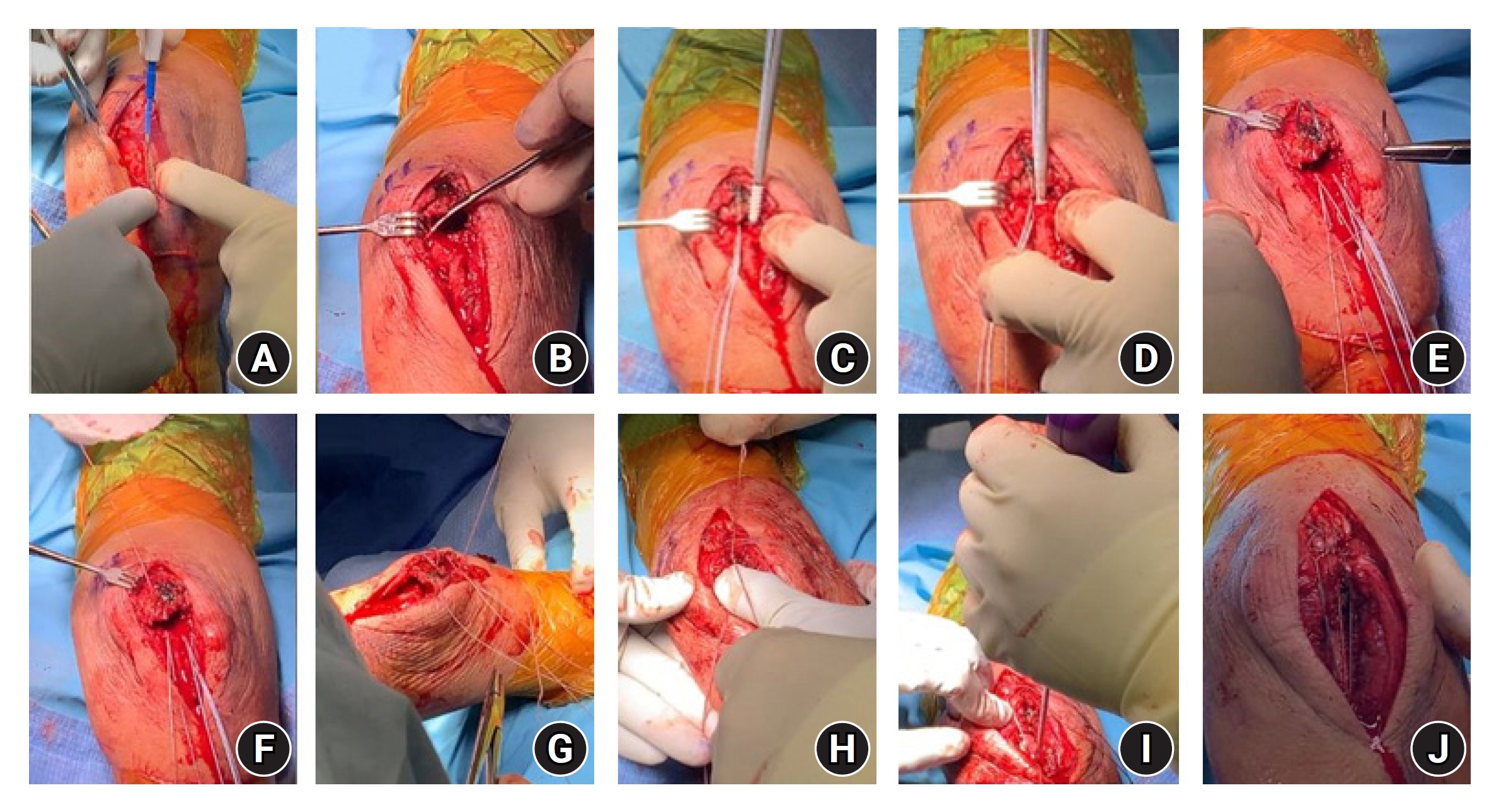
Surgical repair was performed acutely in all cases with nonmetallic suture anchors in a double-row configuration utilizing suture augmentation with the triceps tendon as previously described [11]. In brief, two fully threaded 5.5 mm (or 6.5 mm) biocomposite suture anchors (Arthrex) were placed in the cancellous bone of the proximal ulna at the interface closest to the cortical wall (Fig. 1). The two suture anchors were placed in different spots of the ulna, both are hugging the cortical wall as much as possible for proper fixation. The suture limbs were passed parallelly in a transosseous fashion through the proximal fragment and then through the triceps tendon in a Krackow fashion (Fig. 1). The fracture was then reduced, and two 3.0-mm biocomposite PushLock anchors (Arthrex) were placed distally in the ulnar shaft in a transosseous-equivalent fashion (Fig. 1). The reduction was evaluated visually or with ultrasound to ensure there was no step-off. After surgery, patients were placed in a splint at 30º of flexion for 2–3 weeks. If the patients’ radiographs demonstrated sustained reduction and progressive healing, occupational therapy was initiated to improve active range of motion with the goal of reaching full flexion and extension at 12–16 weeks postoperatively.
Baseline demographic information was obtained through electronic medical records. Patients underwent radiography preoperatively, immediately postoperatively, and at final follow-up. Radiographs were uniformly assessed by the senior surgeon to evaluate osseous union, adequate reduction, and hardware failure. To assess clinical outcomes, patients were contacted via telephone to complete questionnaires regarding their current elbow function. Clinical outcome questionnaires that were used for this purpose included the shortened disabilities of the arm, shoulder, and hand (QuickDASH) score; the Oxford Elbow Score (OES); and the 12-item short form health survey (SF-12). We used descriptive statistics (mean and range) to report on the demographic characteristics of the patients. We also used descriptive statistics to report on the postoperative clinical and radiographic outcomes of the included patients in the study.
Independent t-tests were conducted to compare outcomes between patients under 60 years old and those aged 60 and above, as well as between different sexes. Statistical analysis was carried out using IBM SPSS software version 25.0 (IBM Corp.).
RESULTS
Seventeen patients with a mean age of 65.6 years (range, 22–88 years) at the time of surgery were analyzed after inclusion and exclusion criteria were applied. Functional outcome scores were collected in 12 patients (Table 1) with a mean clinical follow-up time of 5.6 years (range, 2.0–12.9 years). Two patients were unable to be contacted, one patient declined, one patient had dementia, and one patient was deceased.
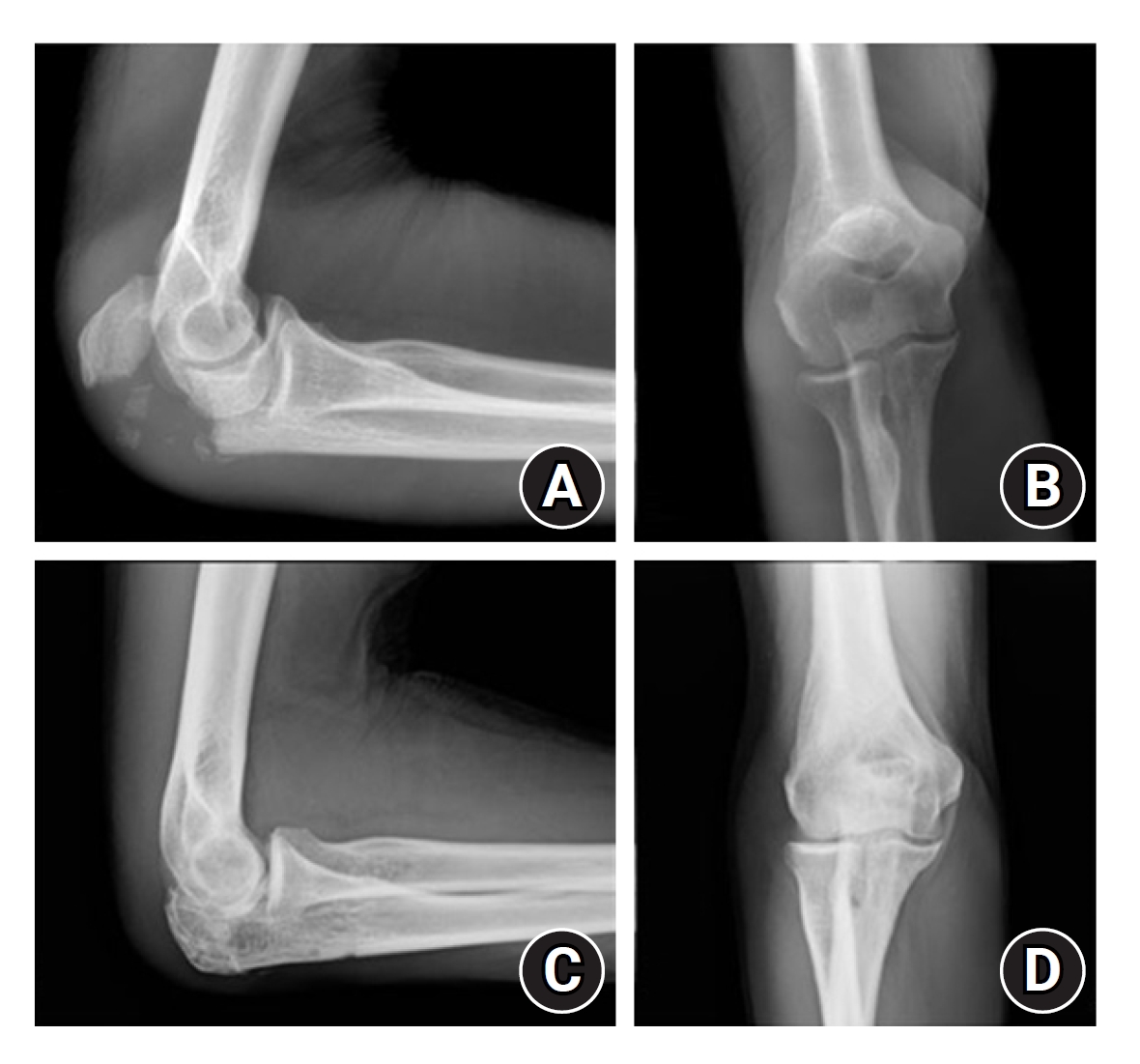
Adequate reduction and fixation were achieved for all patients in the operating room. There were no intraoperative complications noted by the senior surgeon (JAA). One patient developed a postoperative infection that required two reoperations. No hardware failure or fixation failure occurred in this series. At final follow-up, 16 of 17 patients (94.1%) achieved osseous union in an acceptable position (Fig. 2) and one patient had partial union. Despite partial osseous union, this patient had excellent functional outcomes (QuickDASH, 4.8; OES, 46) without additional intervention. No patients in this series had any clinical complaints of symptomatic hardware and none required additional secondary intervention for hardware-related issues.
Excellent long-term patient reported outcomes were achieved according to QuickDASH score and OES. The mean OES was 47.5 (range, 45–48), with nine patients (75%) achieving a perfect score. The mean postoperative QuickDASH score was 3.8 (range, 0–25). One patient (Table 1, patient 2) had a higher QuickDASH score of 25. This patient’s score reflected her recent hip fracture, which was unrelated to her elbow function. This patient had no complaints regarding her elbow function (OES score of 48). The increased disability caused by the hip fracture limited the patient’s ability to perform ‘‘recreational activities” and ‘‘heavy household chores,’’ which were not solely dependent on upper extremity function [12,13]. Patients younger than 60 years achieved equivalent OES (P=0.459) and QuickDASH (P=0.185) to those older than 60 years. There was no difference between genders in OES (P=0.785) or QuickDASH (P=0.536) scores. The mean scores of the SF-12 physical component and mental component were 52±11.8 and 56.6±4.6, respectively. Patient two achieved the lowest scores in both the physical and mental components of the SF-12 survey (Table 1). This is attributed to her recent hip fracture, which impaired her physical health and emotional outlook.
DISCUSSION
Olecranon fractures can pose significant challenges in elderly patients and patients with small fracture fragments. Suture anchors allow sufficient fixation of small fracture fragments that may be insufficiently captured by a plate while minimizing the chance for hardware-related complications. This study demonstrated excellent subjective and objective outcomes, which appear durable with midterm and long-term follow-up. While previously thought to be ideal for elderly patients with osteoporotic bone, younger patients with small fracture fragments achieved excellent outcomes as well. Suture anchor repair does not require implant removal, which is especially advantageous in the elderly orthopedic population. Furthermore, this technique provides greater biomechanical stability in osteoporotic bone due to the addition of a “triceps offloading suture” [14,15].
Traditionally, surgical treatment options for olecranon fractures included plate fixation and tension-band wiring (TBW) [12,16]. Biomechanical studies have suggested that plate fixation is superior to TBW regarding fracture compression [13,17]. However, clinical outcomes have been comparable between the two methods [8]. Duckworth et al. [8] performed a randomized control trial comparing plate fixation to TBW, and they found no differences in DASH or Mayo Elbow Score between plate fixation and TBW or nonunion rates. However, the TBW cohort had a significantly higher reoperation rate following symptomatic hardware removal. Although plate fixation is associated with higher cost for primary surgery, the increased rate of hardware removal associated with TBW results in lower long-term costs [8,18]. Previous studies have shown hardware removal of TBW and plate fixation as high as 82% and 62.5%, respectively [6,19].
The high reoperation rate is especially concerning in the elderly population. TBW is associated with high rates of complications, including fixation loss, nonunion, infection, and reoperation for prominent hardware [5]. Plate fixation has demonstrated lower complication rates but is associated with risk for displacement, wound complications, and reoperation [10]. Suture fixation is superior to these other methods due to decreased risk of complications. As seen in our study, reduction was successfully maintained for all patients. The union rate in our study (94%) is similar to that seen by Campbell et al. [10] with plate fixation. Furthermore, a major advantage of suture anchor repair is that the implanted hardware does not require removal. In the setting of simple olecranon fractures, the use of all-suture fixation techniques has been suggested in the literature. One study by Ernstbrunner et al. [20] showed that tension-band tape had equivalent or superior biomechanical performance compared with other techniques like TBW. Additionally, one randomized control trial protocol, published in 2023, aimed to compare the clinical efficacy and cost-effectiveness of suture fixation versus TBW for simple olecranon fracture fixation in adults [21]. The investigators aimed to provide high-quality evidence for the use of tension suture repair for olecranon fracture fixation [21]. Even though our study utilized suture anchor repair for complex fractures, it provides a foundation for future research exploring suture fixation techniques for olecranon injuries.
A biomechanical study found no difference in displacement rates between TBW and suture anchor repairs for olecranon fractures in patients with osteoporotic bone [22]. Previously, Bateman et al. [11] demonstrated that suture anchor fixation had excellent outcomes in elderly patients. In this updated case series by Bateman et al. [11], two patients had perfect OES 10 years postoperatively. Furthermore, suture anchor fixation had excellent outcomes in both elderly and younger patients [11]. Although our outcomes were studied over a shorter period of time in younger patients, we extrapolate that, based on the combination of current functional outcomes in these patients and the excellent longer outcomes seen in the older patients of this study, patients will have excellent outcomes regardless of age.
In this case series, fracture reduction was successfully maintained in all patients. Osseous union occurred in all but one patient. Previous studies with TBW and plate fixation have shown loss of reduction in as high as 53% of patients [7,19,23,24]. No patients in our current study experienced symptomatic hardware requiring removal. Furthermore, all patients achieved excellent functional outcomes according to OES, with 75% reporting perfect scores. Suture anchor fixation was shown to be an efficient and advantageous surgical method for elderly patients with medical comorbidities, especially compared with other possible techniques like plate fixation, which commonly requires hardware removal.
This study has some limitations. Our case series did not have a large population size and only had a follow-up rate of 70%. However, this case series is the largest to describe outcomes after suture anchor repair. A larger cohort study performed in a randomized fashion is necessary to determine complications and to assess outcomes. Additionally, larger studies are required to assess the functional outcomes of suture anchor repair in patients younger than 60 years. Last, this treatment method was only used in patients with Mayo IIa and IIb fractures, and this technique would likely not be successful in other types of olecranon fractures.
CONCLUSIONS
Suture anchor fixation of displaced olecranon fractures in patients with comminuted Mayo IIa and IIb fractures resulted in excellent midterm functional outcomes. Additionally, this technique resulted in high rates of osseous union without any hardware-related complications or fixation failures. Considering the limitations and complications observed with other treatment modalities used for displaced olecranon fractures, suture anchor fixation is a great option for a complex elbow injury.