INTRODUCTION
Anatomic total shoulder arthroplasty (aTSA) is an effective and reliable treatment for glenohumeral arthropathy [1,2]. aTSA was pioneered by Charles Neer to treat glenohumeral osteoarthritis [3], and the indications have expanded to include osteoarthritis secondary to trauma or inflammatory joint disease as well as complex proximal humerus fractures and shoulder instability [4-7]. Consequently, the incidence and volume of TSA has dramatically increased. Between 2011 and 2017, the annual volume of aTSAs increased by 38.5% and is projected to increase by another 30%–50% by 2025 [8].
Although mid- to long-term outcomes following aTSA have been extensively evaluated, the effects of patient age on long-term clinical outcomes remain an active area of research. Because the vast majority of patients opting for total shoulder replacement are older than 65 years, many papers have been published on the efficacy of TSA in aging populations [9-12]. However, because younger and more active patients are electing aTSA, a transition toward evaluating outcomes within this demographic has been observed in the literature [13-15]. However, the use of aTSA in younger patients remains controversial. Some groups report excellent short- to mid-term outcomes in aTSAs performed on younger-than-average patients [16,17]. In other studies, younger patients who underwent aTSA reportedly had a significantly higher risk of revision and worse clinical outcomes [18-22].
In addition, although clinical outcomes in different age groups have been compared in several studies, the mean follow-up time is relatively short at 3 years [9,20,23]. This limitation is important because long-term implant and revision-free survival are crucial factors for younger patient populations. In the present study, we aim to report on the effects of age on the long-term clinical outcomes following aTSA. We hypothesized that long-term functional and radiographic outcomes are sustained and excellent regardless of age.
METHODS
The Institutional Review Board of the Icahn School of Medicine at Mount Sinai approved this study (No. STUDY-17-00684-CR001). The patients and their families were informed that data from the research would be submitted for publication and provided their consent.
Study Population
This study retrospectively analyzed shoulders of patients who underwent TSA by a single fellowship-trained orthopedic surgeon between December 1992 and May 2018 with a minimum of 2-year follow-up. Due to the heterogeneity in outcomes based on indication following aTSA, we manually excluded all patients who underwent aTSA for rheumatoid arthritis, fracture, post-traumatic arthritis, and avascular necrosis. Initially, 173 shoulders of patients with updated clinical outcome data were included. After applying the exclusion criteria, 119 shoulders were available for analysis.
Surgical Technique
All aTSA procedures were performed using a deltopectoral approach by a single shoulder and elbow fellowship-trained orthopedic surgeon (ELF). Using the subscapularis peel or lesser tuberosity osteotomy techniques, the subscapularis was taken down and repaired at the end of each case. The choices of fixation technique, humeral component, and glenoid component were determined intraoperatively. Generally, cementation was utilized if the bone stock appeared osteopenic or of poor quality, and keeled glenoid was utilized if glenoid morphology or size contraindicated the use of a pegged implant.
Clinical Evaluation
The range of motion and patient-reported outcomes were investigated in this study. Preoperatively and at subsequent follow-up appointments, the surgeon and staff collected clinical outcome data. Forward elevation, external rotation, and internal rotation were assessed using range of motion measures. Internal rotation was measured according to Amroodi et al. [24]. Patient-reported outcomes were evaluated using 24 standardized metrics including the American Shoulder and Elbow Surgeons (ASES) score, Simple Shoulder Test (SST) score, and visual analog scale (VAS) score. The success of the implants was assessed, with revision or removal of the implants considered a failure.
Radiographic Evaluation
Radiographic analysis was performed using immediate postoperative and the most recent follow-up imaging. Images were reviewed and independently scored by two fellowship-trained orthopedic surgeons. Radiographic measures assessed included the acromiohumeral interval (AHI) and glenoid lucency. The AHI was defined as the distance (mm) between the humeral head articular cortex and the inferior acromion. Glenoid lucency was evaluated using the Lazarus classification.
Statistical Analysis
All statistical analyses were conducted using the SciPy 1.6.1 Python package. Continuous variables were evaluated using Student t-test. Categorical variables were evaluated using a chi-square test. Kaplan-Meier survival curve and survival estimates were generated with the associated SciPy 1.6.1 Python package. Univariate linear regression was conducted to evaluate the association of clinical outcome metrics with age. In addition, multivariate linear regression controlling for sex and follow-up interval was conducted to evaluate the association of clinical outcomes with age. P-values were reported for all statistical tests, and P<0.05 was considered statistically significant.
RESULTS
Study Population
A total of 119 shoulders was included in the present study. The indication for inclusion was limited to glenohumeral osteoarthritis. The mean age at surgery, follow-up time, and body mass index were 66.2±8.9 years, 10.8±5.3 years, and 27.3±4.9, respectively. Approximately half of the aTSAs (47.1%) were performed on female patients (Table 1). Patient demographics and outcomes reported include all 119 shoulders. However, in regression analyses, patients with missing data were excluded from the respective model.
Overall Clinical Outcomes
At final follow-up, patients of all ages undergoing aTSA experienced significant and sustained improvements in all primary outcome measures compared with preoperative values. Forward elevation improved from 118.4° to 148.6° (P<0.001). External rotation improved from 20.5° to 55.7° (P<0.001). Internal rotation improved from L5 to T12 (P<0.001). ASES scores improved from 33.9 to 76.54 (P<0.001). SST scores improved from 3.1 to 8.5 (P<0.001). VAS pain scores improved from 6.3 to 2.0 (P<0.001). All clinical outcomes are shown in Table 2.
Radiographic Outcomes
The AHI significantly decreased immediately following surgery to final follow-up (immediate AHI: 10.9±4.5, Final AHI: 8.4±3.7; P<0.001). The distribution of Lazarus scores within the cohort was 0 (n=89), 1 (n=3), 2 (n=4), 3 (n=5) 4 (n=0), and 5 (n=16); scores were unavailable for two patients.
Univariate Analysis
In initial univariate correlation analysis, we evaluated the relationships between age and postoperative outcome measures. Only age was a significant predictor of postoperative internal rotation measurement (β=0.10; 95% confidence level [CI], 0.02–0.18; P=0.011). In addition, although non-significant, a positive correlation was observed between age and postoperative ASES score (β=0.46; 95% CI, −0.02 to 0.94; P=0.059) and VAS pain score (β=−0.05; 95% CI, −0.10 to 0.01; P=0.080). In this univariate analysis, age alone was not a significant predictor of other shoulder function outcome measures such as SST scores, forward elevation, and external rotation.
Multivariate Analysis
In multivariate linear regression analyses, age at the time of surgery was a significant predictor of postoperative outcomes. We used two models, one that controlled for sex and follow-up duration, and a second that controlled for sex, follow-up, body mass index, and ASA status. In the first model, age at the time of surgery was a significant predictor of postoperative outcomes. Postoperative ASES scores (β=0.63; 95% CI, 0.11 to 1.14; P=0.018) and VAS pain scores (β=−0.08; 95% CI, −0.14 to −0.02; P=0.012) were significantly associated with age. In the second model, similar findings showed age at the time of surgery as a significant predictor of postoperative outcomes. Postoperative ASES scores (β=0.69; 95% CI, 0.11 to 1.27; P=0.019) and VAS pain scores (β=−0.08; 95% CI, −0.14 to −0.01; P=0.028) were significantly associated with age. In both multivariate analyses, age was not a significant predictor of SST scores, internal rotation, forward elevation, or external rotation at final follow-up. Additional details regarding the regression analyses are presented in Tables 3-5.
Survival Analysis
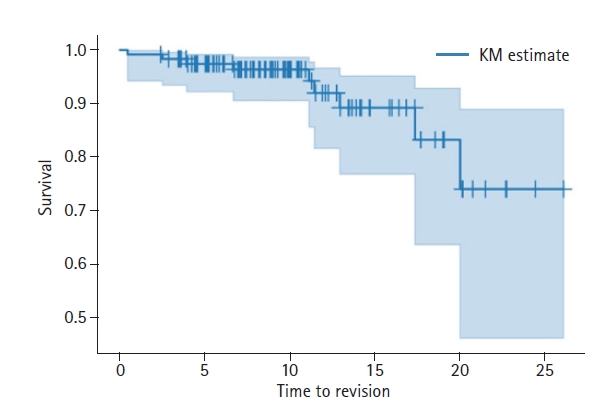
Overall, we observed excellent implant survival over the course of the study (Fig. 1). The 5-, 10-, 15-, 20-, and 25-year survival estimates based on Kaplan-Meier analysis were 97.4%, 96.3%, 89.2%, 83.2%, and 74.0%, respectively. There were nine implant failures with a mean time to failure of 10.7 years. Implant failure was most often secondary to glenoid component loosening (8/9), requiring subsequent arthroscopic glenoid component removal. In addition, Cox regression survival analysis indicated that age (hazard ratio, [HR], 0.98; 95% CI, 0.91 to 1.06; P=0.640) and sex (HR, 0.97; 95% CI, 0.26 to 3.68; P=0.970) of patients undergoing aTSA were not associated with an increased risk of implant failure.
DISCUSSION
Due to the increasing aging population, glenohumeral osteoarthritis is diagnosed more often, with research showing that up to one-third of people presenting with glenohumeral osteoarthritis are older than 60 years [25]. However, there have been studies showing that total shoulder arthroplasty is becoming more common among younger patients [13]. aTSA has been the standard of care procedure in patients who have an intact rotator cuff and sufficient glenoid for prosthetic glenoid implantation, providing patient satisfaction, implant durability, and a low complication rate [26-30]. Prior research has shown that aTSA is an effective surgery to improve shoulder function and shoulder activity level with large effect size [31]. The goal of our study was to determine whether age at the time of surgery affects long-term functional and radiographic outcomes of patients undergoing aTSA. The study cohort included 119 shoulders of patients with an average age of 66.2±8.9 years and a follow-up time of 10.8±5.3 years.
At last follow-up, all patients in the study cohort experienced improvements in range of motion and outcome measures. In previous age-based analyses, older patients appeared to have generally better measured and reported shoulder function [18,20]. However, the available literature also highlights a lack of standardization when comparing age groups, which was a main deciding factor in using regression analysis. Patel et al. [20] observed significantly better outcomes regarding ASES, VAS, and shoulder pain and disability index scores in patients older than 55 years compared with patients younger than 55. Brewley et al. [18] performed a similar analysis that stratified patients into <65 or >65 years of age and reported better ASES and internal rotation scores in the older cohort. A smaller study was performed by Shimada et al., and differences were not observed in range of motion or patient reported outcomes compared with patients >80 and <70 years of age. We observed similar findings in both multivariate models, indicating that, for every 1-year increase in age, ASES score would be 0.63 or 0.69 points higher and VAS pain scores 0.08 or 0.08 points lower. Typically, younger patients have higher physical demands, expectations, and life expectancy compared with the average patient undergoing aTSA [32-34]. This discrepancy in expectations and increased physical demands may contribute to worse patient-reported outcome scores in the younger population because differences in range of motion measurements were not statistically significant.
Generally, in the reported literature, implant survival rates following aTSA are excellent, with an average of 20% of patients experiencing failure or necessitating revision surgery [30]. This is in agreement with overall observations as well with 15-, 20-, and 25-year survival rates of 89.2%, 83.2%, and 74.0%, respectively. In addition, based on Cox regression analysis after controlling for sex and follow-up time, age was not associated with increased risk of implant failure or revision surgery. However, this observation is inconsistent with studies reporting increased revision rates in younger patients. A study by Wagner et al. that included 3,300 aTSAs reported a 3% decrease in revision rate for every 1-year increase in age [22]. Brewley et al. [18] conducted a retrospective analysis on 518 TSAs and observed that patients 65 years of age and younger had a 3.4-fold greater risk of revision than older patients. While the physical demands or activity of younger patients may contribute to early revision, our study failed to show that age alone was responsible for changes in implant failure rates. Last, although Cox regression analysis suggested no association of implant failure risk with age, with only nine total failures in this cohort, our analysis is prone to beta error and limits our ability to conclude specific factors related to failure.
Our study contributes to the literature on the efficacy of aTSA as the standard of care treatment for glenohumeral osteoarthritis. It is one of few studies that has a mean follow-up longer than 10 years that analyzes clinical outcome measures and implant survival by age. The data include nearly three decades of aTSA procedures, which is beneficial due to the length of follow-up but is limited by the advancements in technique, implant technology, and medical imaging. In addition, another limitation in retrospective studies is the limited response rate and medical history available for several patients, which may have influenced regression analysis. For instance, updated patient-reported outcomes, range of motion, and survival data were only available in approximately 25% of patients who underwent aTSA by this surgeon. In the future, use of Elixhauser or Charlson comorbidity scores would be beneficial. Last, the data are from a single surgeon, and the results may not be applicable to the techniques and processes of other surgeons.
CONCLUSIONS
This multivariate regression analysis focused on the impact of age on long-term outcomes following aTSA. When controlling for sex and follow-up duration, older patients were associated with significantly better patient-reported outcome measures. Despite this difference, we noted no significant effects on implant survival.