Pyrocarbon hemiarthroplasty and the shoulder: biomechanical and clinical results of an emerging treatment option
Article information

Abstract
While shoulder hemiarthroplasty is still used to treat young patients with shoulder pathology, the use of this procedure has substantially declined in recent years due to its significant complication profile. Glenoid wear with arthrosis is one of the major postoperative complications following shoulder hemiarthroplasty, and efforts to prevent this complication led many scientists to explore alternative weight-bearing surfaces on arthroplasty implants to decrease joint wear and improve patient outcomes. Pyrolytic carbon, or pyrocarbon, is a material that has better biocompatibility, survivorship, strength, and wear resistance compared to the materials used in traditional shoulder hemiarthroplasty. Pyrocarbon implants have been used in orthopedics for over 50 years; recently, their utility in shoulder hemiarthroplasty has garnered much interest. The purpose behind the use of pyrocarbon in shoulder hemiarthroplasty is to decrease the risk of progressive glenoid wear, especially in young active patients in whom joint preservation is important. Promising survivorship and outcomes have been demonstrated by recent studies, including limited glenoid wear following pyrocarbon hemiarthroplasty. Nevertheless, these clinical studies have been limited to relatively small case series with limited long-term follow-up. Accordingly, additional research and comparative studies need to be conducted in order to properly assess the therapeutic efficacy and value of pyrocarbon hemiarthroplasty.
INTRODUCTION
Shoulder arthroplasty has become increasingly common over the past two decades [1]. While the number of primary reverse total shoulder arthroplasty (rTSA) and primary anatomic total shoulder arthroplasty (aTSA) procedures has increased in recent years, hemiarthroplasty has become less common and its surgical indications have narrowed [2,3]. The procedure remains an important treatment option in a specific subset of patients, primarily young, physically-active individuals with glenohumeral osteoarthritis (GHOA) or avascular necrosis (AVN) of the humeral head [2,4-6]. Compared to other replacement procedures, hemiarthroplasty better preserves glenoid bone stock and typically requires a shorter surgical time [2,4-6].
Despite the advantages of shoulder hemiarthroplasty, there exists a number of potential complications that may compromise outcomes and lead to higher revision rates [7,8]. Joint overload, anterosuperior escape, and glenoid arthrosis are all potential complications [9-13]. The articulation of the metal resurfaced humeral head with the native glenoid can often generate pain, bone erosion, and potential medialization of the joint line [9]. Different studies have explored techniques to minimize the impact of the resurfaced humeral head on the native glenoid with limited success [14,15].
In order to solve this challenge, pyrolytic carbon (pyrocarbon) in the form of pyrocarbon-coated implants or interpositional prosthetic components was introduced as an alternative weight-bearing surface that can decrease glenoid erosion in hemiarthroplasty procedures [16-18]. Early in vitro studies showed promising results, with reduced wear rates compared to other materials [19-21]. Understanding the biomechanical principles and clinical outcomes of pyrocarbon humeral heads is critical to determine its role in the increasingly diverse landscape of shoulder arthroplasty implants. As such, the aim of this review is to evaluate the current use of shoulder hemiarthroplasty, describe the properties of the pyrocarbon material, explore the previous use of pyrocarbon in the surgical setting, and evaluate the utility of this novel technology in shoulder surgery.
SHOULDER HEMIARTHROPLASTY
While aTSA has been shown to provide more consistently successful clinical outcomes for elderly patients with primary GHOA [8,22], the ideal treatment for young, physically-active patients who are at elevated risk of late glenoid component loosening remains unclear. Hemiarthroplasty with or without concentric glenoid reaming (“ream and run”) provides durable clinical improvements without risk of complications related to the glenoid component [15,23-26]. In patients with inadequate bone stock to support a glenoid component, hemiarthroplasty may be preferred [15,23-26]. Patients with AVN without glenoid involvement achieve the most positive outcomes with hemiarthroplasty, whereas relatively poor results are seen with proximal humerus fractures or cuff tear arthropathy [27].
However, higher complication rates are seen with hemiarthroplasty compared to aTSA. Fonte et al. [2] found that the hemiarthroplasty for GHOA had a complication rate of 21.7%, compared to 19.4% among both rTSA and aTSA patients. Hackett et al. [28] reviewed the causes for revision among 359 hemiarthroplasty patients who had indications that included proximal humerus fracture, GHOA, capsulorrhaphy arthropathy, cuff tear arthropathy, and AVN. The most common characteristics of revised hemiarthroplasties were rotator cuff failure, fracture sequelae, and severe glenoid erosion violating the subchondral bone [28]. Severe erosion was present in 35% of cases, with erosion beyond the coracoid base in 4%. While a trend toward rTSA for proximal humerus fractures and those with at-risk rotator cuffs has likely reduced the rates of revision due to cuff failure and fracture sequelae, glenoid wear remains a concern.
Herschel et al. [29] retrospectively reviewed 118 shoulders treated with hemiarthroplasty to explore the rate of postoperative glenoid erosion and arthrosis and to identify possible risk factors. The authors showed that nearly one-third of patients who underwent hemiarthroplasty of the shoulder developed severe glenoid erosion within a mean postoperative time of 2.5 years [29]. The authors also found that osteoarthritis and bone cysts, fatty infiltration of the rotator cuff, and inclination of the prosthetic head were risk factors for glenoid arthrosis in these patients [29]. Specifically, overly horizontal positioning of the prosthetic implant was considered a predictor for erosion as it increases the friction between the implant and the glenoid [29]. Parsons et al. [30] recorded progressive glenoid cartilage wear in eight patients followed for a mean of 43 months, noting a 68% decrease in glenohumeral joint space. The authors also noted lower patient reported outcome scores in those with residual joint spaces smaller than 1 mm compared to those in patients with joint spaces larger than 1 mm [30]. These studies support the potential of glenoid wear following shoulder hemiarthroplasty and the resulting limitations placed on the use of this procedure.
PYROCARBON HISTORY AND COMPOSITION
Pyrocarbon was originally developed in the late 1960s as a strong, durable, and wear-resistant coating for nuclear fuel particles [31]. Pyrocarbon is a form of pure elemental carbon similar to graphite and exists in a disordered crystalline structure composed of randomly oriented continuous crystalline array regions with a sheet layer spacing of approximately 0.348 nm [32]. Due to the small size of these arrays and their random orientation in space, bulk pyrocarbon has isotropic mechanical and physical characteristics. Disorder between adjacent sheets increases the strength of pyrocarbon compared to the more organized crystalline structure of graphite [33,34].
After its initial development, pyrocarbon was modified at the University of Wisconsin to have increased biocompatibility and survivorship in the biological environment for use in long-term cardiovascular implants [31]. Since then, pyrocarbon has been used for over 35 years in various applications for upper extremity orthopedic prosthetics composed of a graphite core with a pyrolytic carbon coating up to 1 mm thick (Fig. 1) [33]. The graphite core defines both the size and the shape of the implant, while the outer pyrocarbon coating provides strength, longevity, and resistance to wear and fatigue [33,35,36]. Tungsten is mixed into the graphite portion to impart radiopacity, while the pyrocarbon layer is radiolucent. This results in a radiolucent halo around the bright white radiopaque core on radiographs [32,37]. Different types of pyrocarbon implants exist, especially in the shoulder; and several clinical reports describe their use for treatment of challenging shoulder pathologies in young patients (Figs. 2 and 3) [17,18].
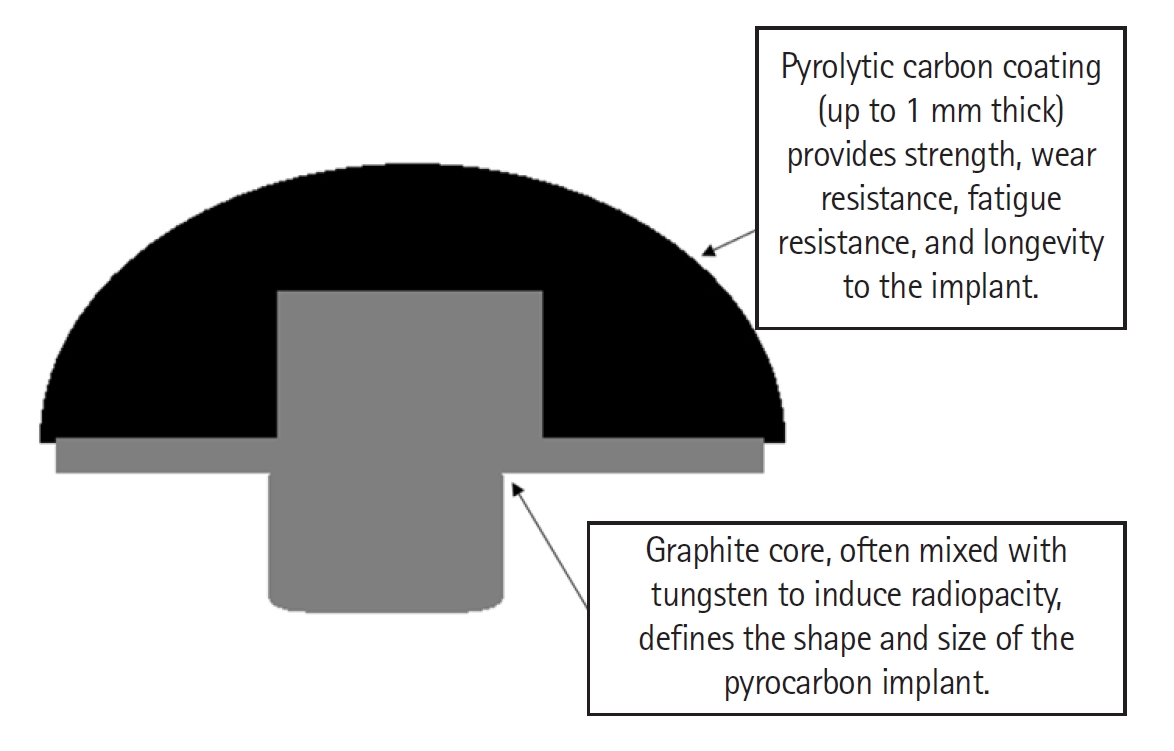
Pyrolytic carbon implant showing the graphite core that defines the implant shape and size and the pyrolytic carbon coating that adds strength and longevity.

An X-ray image of a pyrocarbon hemiarthroplasty implant.
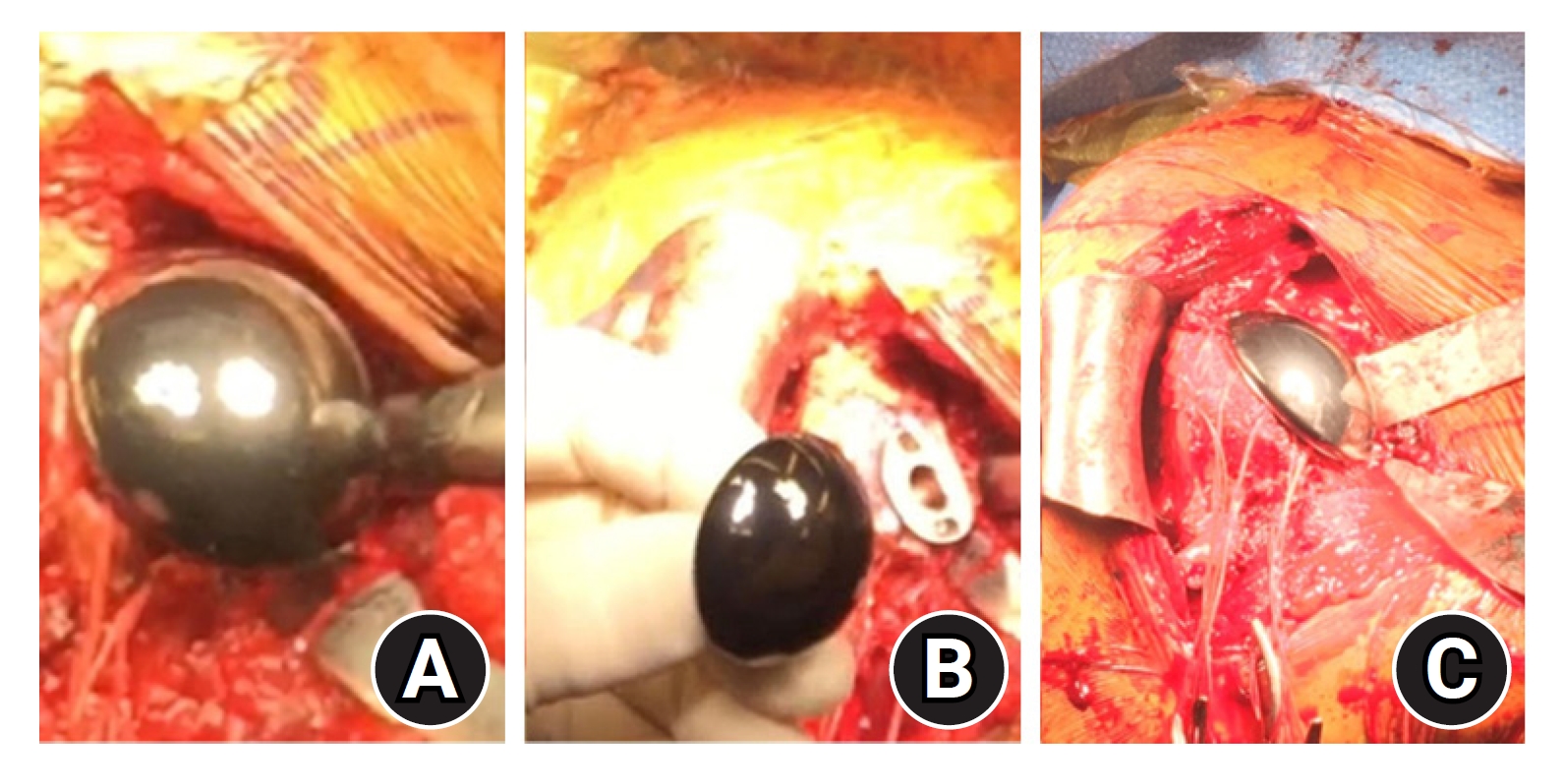
(A-C) Operative implantation of a pyrocarbon hemiarthroplasty implant.
The material is made by heating hydrocarbons to temperatures above 1,200 ºC in the absence of oxygen, the product of which is then deposited onto a graphite core by chemical vapor deposition [33,38,39]. Most carbon-based materials are compatible with the biologic environment, and the same applies for pyrocarbon. However, the crystallographic structure formed by this production process imparts mechanical and tensile strength not demonstrated in all carbon materials. This provides pyrocarbon with prominent fatigue and crack resistance, a beneficial trait for use in long-term implants [40,41].
Pyrocarbon has both a similar density and Young’s modulus to bone, which allows implants to be biomechanically compatible and for minimal stress shielding at the bone-prosthesis interface. Alongside the strength provided by its crystalline structure, this structure also allows pyrocarbon implants to have good durability and wear resistance [42,43]. In the clinical setting, research analyzing fatigue failure has shown promising results over 30 years of use. For example, the use of pyrocarbon in heart valve prostheses has eliminated wear as a mode of failure [44-46].
PYROCARBON AND OTHER MATERIALS
As more patients undergo shoulder arthroplasty at younger ages, there is a need for durable and biocompatible implants to reduce the risk of long-term complications such as component loosening, osteolysis, and polyethylene wear [21,47-49]. In the hemiarthroplasty setting, the articulating surface of the implant is in contact with the native joint surface or a reamed surface in the case of ream and run. Glenoid wear occurs over time through abrasion, adhesion, fatigue, third body wear, and corrosion [21,50].
Several laboratory studies have indicated that pyrocarbon is less damaging to cartilage compared to traditional implant materials. Animal studies using pyrocarbon for joint prostheses in comparison to cobalt-chromium (CoCr) and titanium alloy have shown better tolerance and significantly less cartilage wear [51]. Although the reason remains uncertain, this preservation of cartilage reduced the amount of joint space narrowing and pain caused by long-term use [51]. Pyrocarbon may also have a role in increased production of type II collagen, leading to formation of a cartilaginous matrix at the articulating surface; however, there are limited data on the clinical benefit [21,52]. Over time, when pyrocarbon was brought into contact with the bony surface of the native joint, less damage than with traditional metal alloys was observed [32,53]. Bone volume loss seen in lab testing from CoCr alloys was approximately 100 times greater than that seen with pyrocarbon, indicating that joint preservation is more likely with a pyrocarbon humeral head implant [32].
In an in vitro study by Klawitter et al. [54], pyrocarbon showed more favorable wear characteristics than CoCr. Using a simulator applying 756 N of applied load to mimic demand conditions of a shoulder hemiarthroplasty patient, damage to the articular surface was observed after 320,000 cycles with CoCr, compared to over 5 million cycles with pyrocarbon [54]. Pyrocarbon also demonstrated 30 times lower linearized bone penetration, bone loss volume rate, and changes to surface roughness compared to CoCr, suggesting that pyrocarbon may be a durable treatment option in the younger patient population [54,55]. In addition, lower production of wear-related particles can potentially reduce risk of osteolysis and aseptic loosening, which occurs in approximately 4% of hemiarthroplasty cases requiring revision [28,32,37]. Considering the biocompatibility and less caustic relationship with cartilage and bone, pyrocarbon is a promising alternative for hemiarthroplasty implants that require long lifespans [32].
PYROCARBON HEMIARTHROPLASTY OF THE SHOULDER
The earliest clinical use of pyrocarbon implants in orthopedics was in 1968 to treat thumb carpometacarpal arthritis, and the utility of pyrocarbon implants was expanded to treat other small joint conditions of the hand and other areas in the body [56]. Positive outcomes from pyrocarbon hemiarthroplasty emerged for different conditions affecting small joints in the hand and were evident through reports of prominent improvements in pain, function, and grip strength [57,58]. Nevertheless, some reports highlighted concerns for procedure-related complications, including postoperative arthritis, component loosening and dislocation, and nerve impingement [59]. As such, wide adoption of pyrocarbon implants has been limited to hand surgery, possibly due to its complication profile and higher costs [60,61]. Pyrocarbon implants have also been used in the lower limb, as reported by Bernasek et al. [62], who conducted a pilot study of pyrocarbon hemiarthroplasty on two groups of patients diagnosed with either hip fracture or femoral head osteonecrosis. The authors reported a significantly higher rate of revision in the osteonecrosis group compared to the fracture group, mainly due to acetabular wear and groin pain, indicating mixed results and equivocal benefit of the pyrocarbon implant [62]. As such, application of pyrocarbon in different joints, while promising, did not lead to a convincing integration into standard arthroplasty practice.
In the setting of shoulder hemiarthroplasty, pyrocarbon-coated implants and pyrocarbon inter-positional humeral head prostheses have been developed, and early clinical results have been reported. Cointat et al. [16] reported the survivorship and short-term outcomes of 64 consecutive patients who underwent pyrocarbon hemiarthroplasty for GHOA, with an average follow-up of 33 months. Survival rate of the prosthesis was 92%, with five patients undergoing revision conversion to total shoulder arthroplasty: one patient was converted to aTSA due to painful glenoid erosion, and four patients were converted to rTSA due to postoperative rotator cuff deficiency [16]. The authors also reported that approximately 91% of the patients returned to work and 88% of the patients returned to sports [16]. Similarly, a study by Tsitlakidis et al. [63] explored the survival rates and clinical outcomes of 16 patients ranging from 29 to 65 years in age, with an average follow-up of 24 months. The patients had undergone a pyrocarbon hemiarthroplasty of the shoulder due to GHOA, rheumatoid arthritis, or AVN [64]. At follow-up, the authors reported an arthroplasty survival rate of 94%, and significant improvements in Constant scores and pain scores were reported. Only one revision surgery was necessary due to a periprosthetic fracture [63]. Another prospective study by Garret et al. [64] followed 65 patients who underwent pyrocarbon hemiarthroplasty of the shoulder for GHOA, AVN, or rheumatoid arthritis. At a mean follow-up of approximately 26 months, the authors reported improvement in mean Constant score from 31 preoperatively to 74 and Single Assessment Numeric Evaluation scores from 32 to 78 at most recent follow-up [64]. The authors also conducted radiographic analyses at 2-year follow-up and reported no glenoid erosion in 86% of the patients; however, six patients showed progressive glenoid erosion and 3 showed thinning of tuberosities [64].
While early clinical outcomes are promising, there are limited mid- and long-term data available. A study by Hudek et al. [65] examined the use of a free pyrocarbon-coated interposition arthroplasty in the shoulders of 10 patients for treatment of advanced collapse of the humeral head following AVN. At a mean follow-up of 3.6 years, the authors reported excellent improvements in quality of life and function as demonstrated by significant improvements in clinical outcome scores that are comparable to those of aTSA. These improvements comprised a 63-point increase in Constant scores and 47-point increase in Disabilities of the Arm, Shoulder and Hand (DASH) scores [65]. On radiographic analyses, the authors reported 1.4 mm mean glenoid erosion, –0.8 mm thinning of tuberosities, and 2 mm superior displacement of implant [65]. Another study by McBride et al. [66] used a national joint replacement registry to explore the outcomes of patients younger than 55 years who underwent primary shoulder arthroplasty for GHOA. The authors compared the outcomes of 163 patients who underwent pyrocarbon humeral resurfacing hemiarthroplasty to those of 163 patients who underwent CoCr humeral resurfacing and 67 patients who underwent metal stemmed hemiarthroplasty [66]. At a mean follow-up of 6 years, revision rates were 17.1% for metal hemi-resurfacing, 17.5% for metal stemmed hemiarthroplasty, and 8.9% for pyrocarbon hemi-resurfacing, with pain, prosthesis fracture, and infections as the key reasons for revisions [66]. No pyrocarbon hemi-resurfacing cases were revised for glenoid erosion, further supporting the use of this implant for young GHOA patients [66].
Despite promising clinical outcomes, a few studies have highlighted concerns regarding relatively high revision rates of the implant [17,67]. Hirakawa et al. [17] reported outcomes of 10 patients who underwent pyrocarbon interposition arthroplasty of the shoulder. Patients included were younger than 60 years with either AVN of the humeral head, GHOA with Walch type B glenoids, or secondary severe osteoarthritis [17]. Of the 10 patients, five required revision surgery to rTSA at a mean follow-up time of 60 months due to poor clinical outcomes based on Constant and Subjective Shoulder Value scores [17]. The remaining five patients had significant improvements in clinical outcome scores, though their follow-up duration was less than 35 months [17]. That study, while limited by a small population, expressed concern over the longevity of pyrocarbon implants in the shoulder [17]. Moreover, Pangaud et al. [67] reported a case of a pyrocarbon humeral head resurfacing implant fracture that occurred without any clear trauma or dislocation at 6 years post-implantation. The authors report that the patient presented with pain and pseudoparalysis before imaging studies confirmed fracture of the implant [67]. The report expressed concern regarding the fragility of the implant [67]. A summary of the reported studies is presented in Table 1 [16,17,63-67].
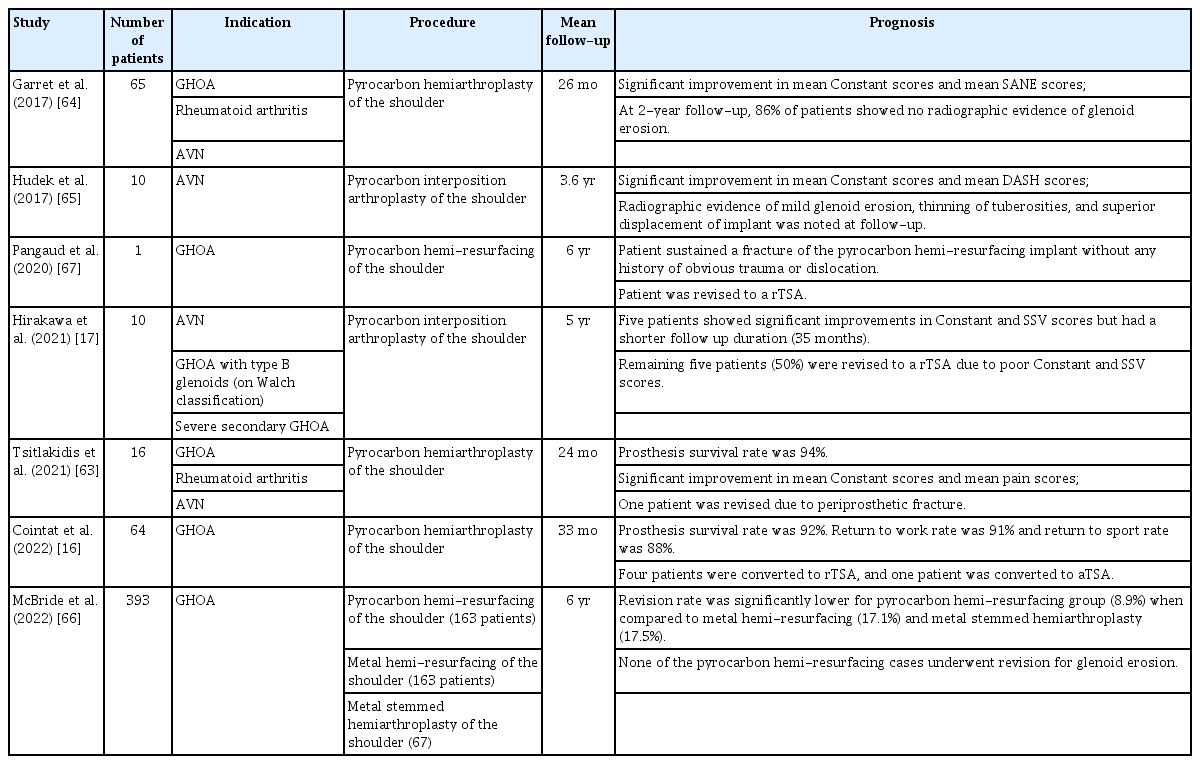
Summary of studies reporting on the outcomes of pyrocarbon-coated hemiarthroplasty of the shoulder
RECOMMENDATIONS
While in vitro research provides a strong basis for use of pyrocarbon implants, clinical results are limited. These implants show promise for young, physically active adults with AVN or humeral head arthrosis and a preserved glenoid. Pyrocarbon implants with ream and run may have future clinical use, though literature in this context is currently unavailable.
As such, additional research with longer-term follow-up is needed to assess the safety, durability, and clinical results of this implant. Large comparative studies and clinical trials should be conducted in order to determine the advantages of this treatment option compared to other common procedures for young patients with GHOA including traditional hemiarthroplasty, ream and run, and aTSA.
CONCLUSIONS
The concept behind the use of pyrocarbon in replacement procedures was to create a prosthesis that has better biocompatibility, survivorship, strength, and wear resistance compared to prostheses of other biomaterials. Pyrocarbon heads are made of a graphite core with pyrolytic carbon coating and have been used in orthopedics for over 50 years. While mostly associated with hand and wrist replacement procedures, pyrocarbon prostheses have been recently used in shoulder surgery, specifically shoulder hemiarthroplasty in young patients at risk of progressive glenoid wear. Biomechanical and early clinical results suggest promising short-term survivorship, clinical outcomes, and limited glenoid wear. However, clinical studies have been limited to relatively small case series, and long-term outcomes are not yet available. As such, additional research on this technology is warranted to establish its role in the growing landscape of shoulder arthroplasty implants.
Notes
Author contributions
Conceptualization: MYF, JS, PB, MRC, JAA. Investigation: MYF. Methodology: MYF. Supervision: JAA. Validation: JAA. Project administration: JAA. Writing – original draft: MYF, JS, PB, MRC. Writing – review & editing: MYF, JS, PB, MRC, JAA.
Conflict of interest
JAA would like to disclose the board member/committee appointments for American Shoulder and Elbow Society, Pacira. Additionally, financial support for this article is disclosed in the Funding section below. Apart from the disclosed financial support and the aforementioned board member/committee appointments, no other potential conflicts of interest relevant to this article have been reported.
Funding
JAA would like to disclose royalties from Djo Global, Zimmer-Biomet, Smith And Nephew, Stryker, Globus Medical, Inc.; research support as a PI from Lima Corporation - Italy, Orthofix, Arthrex, Oref; royalties or financial or material support from Wolters Kluwer.
Data availability
None.
Acknowledgments
None.