INTRODUCTION
Stiffness of the shoulder joint is frequently encountered after arthroscopic rotator cuff repair (ARCR), with reported incidence ranging from 4.9% to 39% [1-3]. Although the pathophysiology of stiffness following ARCR is not well understood, it has been attributed to postoperative immobilization and adhesions and contracture of the articular capsule and surrounding soft tissues that develop after the procedure [3,4]. Despite successful ARCR, postoperative stiffness may significantly affect shoulder function and lead to patient dissatisfaction.
Although various treatment methods such as oral medications, physical therapy, and arthroscopic adhesion release have been suggested to treat post-ARCR stiffness and can be effective, they often have unpredictable outcomes [5-7]. Frequently used for improving pain and function after ARCR [8], corticosteroid injection (CSI) administered to the affected glenohumeral joint has been proposed to effectively treat post-ARCR stiffness [9,10]. However, evidence is lacking regarding the efficacy of CSI to treat post-ARCR stiffness and the optimal dosage, timing, and regimen of CSI to treat postoperative stiffness. In a prospective study of 74 patients who developed post-ARCR stiffness, Kim and Jung [9] reported that intra-articular CSI administered at 6 weeks postoperatively to treat shoulder stiffness achieved significant improvements in pain and range of motion (ROM) at 3 months postoperative without compromising repair integrity. Similarly, Ha et al. [10] reported better pain and functional outcomes in 45 patients with post-ARCR stiffness who were administered single CSI at 4 or 6 weeks postoperative compared to 72 control patients who did not receive any injection at the end of 3 months. CSI may be associated with risk of retears, which limits its use [11].
Data on the efficacy of CSI to treat post-ARCR stiffness are lacking, and the few studies that have evaluated such outcomes were conducted in small patient groups with or without appropriate control groups for comparison [9,10]. Hence, the aim of this prospective, multicentric, case-control study was to analyze and report the efficacy and complications of single-dose CSI administered at 6 weeks postoperative to treat post-ARCR stiffness in a large patient cohort at the end of 18 months of follow-up. We hypothesized that single-dose CSI administered at 6 weeks postoperative to treat post-ARCR stiffness would significantly improve pain and function without significant increase in the incidence of complications such as retears compared to patients who did not receive CSI.
METHODS
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. As the study was conducted in private setups, institutional review board or ethics committee approval was not taken. The same has been communicated to and approved by the editor and reviewers. Written informed consent was obtained from all individual participants included in the study.
Study Design
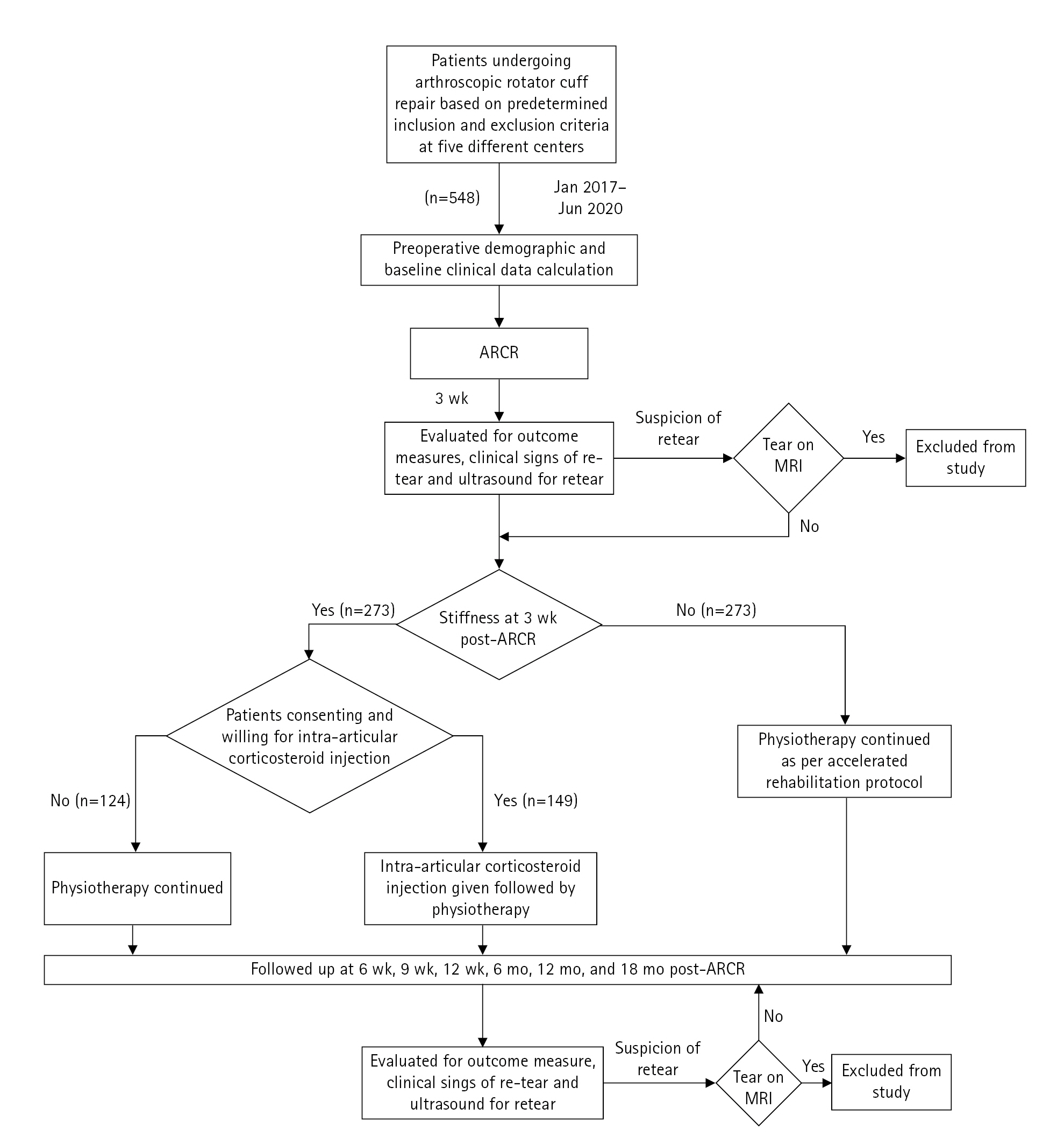
This prospective, multicentric, case-control study was conducted across five centers and included 548 consecutive patients who underwent ARCR between January 2017 and June 2020.
Patient Population
The inclusion criterion for the study was clinical and radiological diagnosis of isolated full-thickness rotator cuff tear not more than 1 year prior. The exclusion criteria were conversion of a partial tear of the rotator cuff to a full tear intraoperatively before repair; labral repair along with rotator cuff repair; history of previous intra-articular steroid injection; history of surgery of the affected shoulder, ipsilateral elbow, or ipsilateral wrist; adhesive capsulitis preoperatively; neuromuscular pathology of the ipsilateral side; complications such as retear or infection during the follow-up period; and loss to follow-up.
Surgical Technique
All patients included in the study underwent ARCR in a double-row configuration with the medial row fixed by two double-loaded suture anchors and the lateral row by a single SwiveLock suture anchor, further tightening the repair. All patients operated on for rotator cuff tear and who were aged >50 years underwent biceps tenotomy as a prophylactic measure to reduce anterior shoulder pain and to encourage faster rehabilitation [12,13]. Postoperatively, all patients were advised to maintain immobilization of the shoulder joint for 3 weeks. At the end of 3 weeks, patients began a three-stage rehabilitation protocol. Passive mobilization, pendulum exercises, and capsular stretching were administered for 1 week. Active-assisted ROM and mobilization exercises were administered for the next 2 weeks, followed by strengthening exercises for the next 4 weeks once target ranges had been achieved.
Patients who did not improve beyond 30┬░ and 40┬░ of external rotation (measured with the arm at the side) at the end of 6 weeks post-surgery (3 weeks after starting physiotherapy) and who showed signs of joint reactivity and pain were diagnosed with post ARCR stiffness. If pain irritability was present, the patient was diagnosed with post ARCR stiffness and was counselled for steroid injection in the glenohumeral joint, explaining the risks and benefits of the procedure. The rationale behind administering CSI at the end of 6 weeks post-surgery was to allow enough time to pass postoperatively to minimize the risk of infection or retear. Thus, CSI can be administered before patients develop tightness in the anterior capsule. Patients who provided consent for the injection were administered 2 mL (80 mg) of depot methylprednisolone mixed with 5 mL of 2% plain lignocaine in the glenohumeral joint under aseptic conditions on an outpatient basis the same day. Patients were tested for lignocaine sensitivity before the injection. Rehabilitation was resumed the following day (Fig. 1). Patients who did not consent to the injection were continued on physical rehabilitation therapy with oral analgesics as required.
Study Outcome Measures
Pain intensity in all patients was measured using the visual analog scale (VAS), and functional outcomes were measured using the Constant Murley Shoulder Score (CMSS) (including strength testing) [14] and time to return to activities of daily living (ADLs). All patients were assessed for complications such as infection and retear during follow-up. If there was any suspicion of a retear, the patient underwent magnetic resonance imaging (MRI) to confirm the status of the rotator cuff. Patients were followed up at 6 weeks, 9 weeks, 12 weeks, 6 months, 12 months, and 18 months postoperatively.
Statistical Analysis
All statistical analyses were performed using IBM SPSS ver. 24 (IBM Corp.). Baseline demographic and clinical variables of mean age; sex distribution; side affected; mean duration of preoperative symptoms; mean preoperative VAS score; and mean preoperative active shoulder abduction, flexion, internal rotation, and external rotation ROMs were compared between CSI and non-CSI groups. Function as measured by CMSS, pain intensity as measured by VAS score, mean duration to return to ADLs post-stiffness, and complications such as retear and infection rates were compared between the CSI and non-CSI groups at 6 weeks, 9 weeks, 12 weeks, 6 months, 12 months, and 18 months postoperatively to determine the efficacy of CSI. Any patient who developed a complication such as retear or infection or was lost to follow-up during the 18 months of follow-up was excluded from data analyses, which compared CMSS, VAS score, and mean duration to return to ADLs. Continuous data were compared using t-tests, and categorical data were compared using Fisher's test. The P-values <0.05 were considered statistically significant.
RESULTS
A total of 273 patients (50%) developed signs of stiffness at the end of 6 weeks post-surgery. Of these, 149 patients (54.5%) consented to intra-articular CSI (CSI group), and the remaining 124 patients (45.5%) chose not to undergo CSI (non-CSI group). The demographic details of these patients are summarized in Table 1. There were no significant differences in mean age (P=0.49); sex distribution; mean duration of preoperative symptoms (P =0.15); mean VAS score (P=0.07); and mean active shoulder abduction (P=0.72), flexion (P=0.31), internal rotation (P=0.29), and external rotation (P=0.35) ROMs between groups (Table 1). However, a significantly greater percentage of dominant side shoulders (P =0.006) underwent ARCR surgery in the non-CSI group compared to the CSI group (Table 1).
During follow-up, the incidence of retears in all patients who developed post-ARCR stiffness in the current study was 7.5% (21/273 shoulders). One patient developed retear at 9 weeks, 10 patients at 12 months, and 10 patients at 18 months post-ARCR stiffness. The incidence of retears of 6% (9/149 shoulders) in the CSI group was not significantly different (P=0.36) compared to the incidence of retears of 9.5% (12/124 shoulders) in the non-CSI group. Seven patients were lost to follow-up in the CSI group, and eight patients were lost to follow-up in the non-CSI group. Hence, clinical outcomes were analyzed in 133 patients in the CSI group and 104 patients in the non-CSI group after excluding patients who developed retear during follow-up.
During follow-up, the mean CMSS was not significantly different at 6 weeks (P=0.89) between the CSI and non-CSI groups but was significantly greater in the CSI group than the non-CSI group at 9 weeks (P<0.001), 12 weeks (P<0.001), and 6 months (P<0.001) (Table 2). However, the mean CMSS was not significantly different between groups at 12 months (P=0.11) or 18 months (P=0.11) (Table 2). The mean duration to return to ADL of 11.5┬▒0.8 weeks in the CSI group was significantly shorter (P<0.001) than the mean duration of 16┬▒2.2 weeks in the non-CSI group.
Similarly, during follow-up, after diagnosis of post-ARCR stiffness, the mean VAS score was not significantly different at 6 weeks (P=1.00) between groups but was significantly lower in the CSI group at 9 weeks (P<0.001), 12 weeks (P<0.001), and 6 months (P<0.001) (Table 2). However, the mean VAS score was not significantly different between groups at 12 months (P=0.05) or 18 months (P=0.05) (Table 2).
DISCUSSION
We demonstrated that single-dose CSI administered at 6 weeks postoperatively to treat post-ARCR stiffness significantly improved pain and function up to 6 months of follow-up without significant increase in the incidence of retear compared to patients who did not receive CSI. However, the two groups experienced similar pain and function with no significant difference in CMSS or VAS score at 12 and 18 months of follow-up. Our results were similar to those of Ha et al. [10], who reported significant impacts on pain and function for up to 3 months between CSI and non-CSI groups. However, that was a retrospective study of a relatively small number of patients (45 patients in the CSI group and 72 patients in the non-CSI group).
The incidence of postoperative stiffness in patients undergoing ARCR surgery in our study was 49.8% (273/548 patients), which was higher than the 39% reported in the literature [1-3,15]. A possible explanation for the higher incidence of post-ARCR shoulder stiffness in the current study could be the higher percentage of female patients, lower mean patient age (<56 years) with lesser opportunity to experience tendon degeneration, and lack of acromioplasty in most patients undergoing ARCR, all of which have been reported as risk factors for post-ARCR stiffness [15].
Considering the debilitating effect of postoperative stiffness, its timely diagnosis and adequate intervention are vital for satisfactory rehabilitation and early return to ADLs. For this, we injected a combination of 2 mL (80 mg) methylprednisolone acetate and 5 mL of 2% plain lignocaine into the glenohumeral joint as soon as the patient showed early signs of stiffness (6-week follow-up). We implemented 3 weeks of immobilization post-surgery, followed by mobilization physiotherapy of the affected shoulder joint to prevent postoperative stiffness due to reasons such as capsular inflammation and soft tissue adhesion and to improve patient compliance as recommended by evidence-based guidelines [16-18]. Based on a previous study [9] and the surgeonsŌĆÖ experience, we waited for 6 weeks postoperative, which included 3 weeks of physical therapy, to clinically identify early signs of post ARCR stiffness.
Corticosteroids primarily reduce pain and improve function through anti-inflammatory effects by inhibiting the phospholipase A2 enzyme and reducing the production of inflammatory mediators such as prostaglandins and leukotrienes [19]. Postoperative CSI following ARCR surgery has previously shown good results [8-10]; however, the timing and number of these injections are a matter of debate. We administered a single CSI at 6 weeks postoperative to consenting patients. The rationale behind the timing of the injection involved circumventing the natural initial inflammatory period necessary for healing of the injury and minimizing the chances of infection as shown previously [20]. Even though the functional scores at 12 and 18 months of follow up were similar between the two groups, pain (VAS score) and function (CMSS) improved significantly in the CSI group during the initial 6 months compared to the non-CSI group. Similarly, the time to return to daily activity was significantly shorter in the CSI group than the non-CSI group. We postulate a direct correlation between pain subsidence following injection and better compliance with the physiotherapy regime as a reason for early return of ROM and quicker return to ADL since there were no significant differences in the baseline characteristics of the two groups.
It has been postulated that intra-articular CSI increases the risk of recurrence of tear, failure of fixation, or tear at a different site due to localized muscle and tendon weakening after attenuation of the strength of the collagen fibers [21,22]. However, a recent systematic review by Puzzitiello et al. [8], which analyzed seven studies comprising 5,528 patients, concluded that postoperative CSI following primary rotator cuff repair is safe and does not increase the rate of retear or infection if administered after the first postoperative month. Similarly, the incidence of retear in the CSI group in the current study was only 6%, similar to the incidence in the non-CSI group and to those reported in previous studies [9,23].
Our study is one of the largest prospective, multicentric, case-control studies to investigate the efficacy of single-dose CSI administered at 6 weeks postoperative to treat post-ARCR stiffness. However, this study has limitations. First, the non-randomization of the CSI and non-CSI groups may have introduced selection bias, which may have influenced the results of the study. Second, the indication for injection was based on the presence of shoulder pain and stiffness, which were determined clinically at around 6 weeks post-ARCR surgery. This could have introduced diagnosis bias, especially in a multicentric setup. In addition, the effect of CSI on the integrity of the repaired rotator cuff should have been evaluated at each follow-up visit using MRI before and after the injection. However, this could not be performed given the increased cost of investigation to the patient, although cases with clinically suspected rotator cuff retear during follow-up underwent MRI for this reason.
In conclusion, this study demonstrated that single-dose intra-articular CSI administered at 6 weeks postoperative to treat post-ARCR stiffness significantly improved pain, function, and duration of return to ADLs without increasing the risk of retear compared to patients who did not receive intra-articular CSI. Hence, single-dose intra-articular CSI administered at 6 weeks postoperative is safe and effective for treating post-ARCR stiffness.