Regional nerve blocks for relieving postoperative pain in arthroscopic rotator cuff repair
Article information

Abstract
Rotator cuff tear is the most common cause of shoulder pain in middle-age and older people. Arthroscopic rotator cuff repair (ARCR) is the most common treatment method for rotator cuff tear. Early postoperative pain after ARCR is the primary concern for surgeons and patients and can affect postoperative rehabilitation, satisfaction, recovery, and hospital day. There are numerous methods for controlling postoperative pain including patient-controlled analgesia, opioid, interscalene block, and local anesthesia. Regional blocks including interscalene nerve block, suprascapular nerve block, and axillary nerve block have been successfully and commonly used. There is no difference between interscalene brachial plexus block (ISB) and suprascapular nerve block (SSNB) in pain control and opioid consumption. However, SSNB has fewer complications and can be more easily applied than ISB. Combination of axillary nerve block with SSNB has a stronger analgesic effect than SSNB alone. These regional blocks can be helpful for postoperative pain control within 48 hours after ARCR surgery.
INTRODUCTION
Patients with shoulder problems are commonly encountered in the medical field. Among them, rotator cuff tear is the most common cause in patients of middle age and older. [1]. A rotator cuff tear causes significant pain and dysfunction of the shoulder and should be treated properly [2]. In the United States, over 250,000 rotator cuff repairs are performed annually, and arthroscopic repairs have increased in frequency [3]. Arthroscopic rotator cuff repair (ARCR) can be performed in inpatient or outpatient settings, but there is concern about postoperative pain in the early period [4]. Generally, an arthroscopic procedure induces less postoperative pain than an open procedure. Warrender et al. [5] found that arthroscopic repair resulted in significantly decreased postoperative pain and better functional outcomes. Stiglitz et al. [6] showed that postoperative pain after arthroscopy peaked at postoperative day 1. Early postoperative pain after arthroscopic shoulder surgery is a major source of concern for patients and surgeons [7]. Some studies reported that severe postoperative pain was observed in the first 48 hours after rotator cuff repair [8]. Early proper management of postoperative pain is important for better outcomes and can reduce costs and the hospitalization period as well as aid in recovery, including rehabilitation and nourishment [4].
Postoperative pain can be the result of not only direct destruction of tissue, including skin, synovium, capsule, and bone, but also stimulation of pain receptors. During an operation, tissue trauma with direct peripheral nerve injury can induce inflammation. This inflammation can result in over-sensitization of pain receptors, increasing the importance of early postoperative pain relief [9]. There are many methods for controlling postoperative pain, including patient-controlled analgesia (PCA), opioids, interscalene block, and peripheral nerve block [10]. PCA and opioids have a systemic effect and might not control pain adequately because of side effects like nausea, vomiting, and sedation. The interscalene block is commonly used and effective for shoulder arthroscopy [11]. This type of block has a strong effect on analgesia, but there are side effects like rebound pain in 5%–10% of cases [12]. As the interscalene block also can affect the phrenic nerve, it can lead to pulmonary problems like respiratory distress or diaphragmatic paresis [13]. Recently, the peripheral nerve block, like the suprascapular nerve block (SSNB) and axillary nerve block (ANB), has been utilized and has worked relatively well at controlling pain. There have also been studies that analyzed the effects of regional blocks (Table 1). Among these studies, randomized controlled trials are described in Table 2 [14-24]. In this review, we analyzed the effect of interscalene brachial plexus block (ISB), SSNB, and ANB.
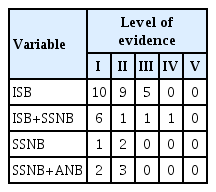
Studies that analyzed the effects of regional blocks in arthroscopic rotator cuff repair
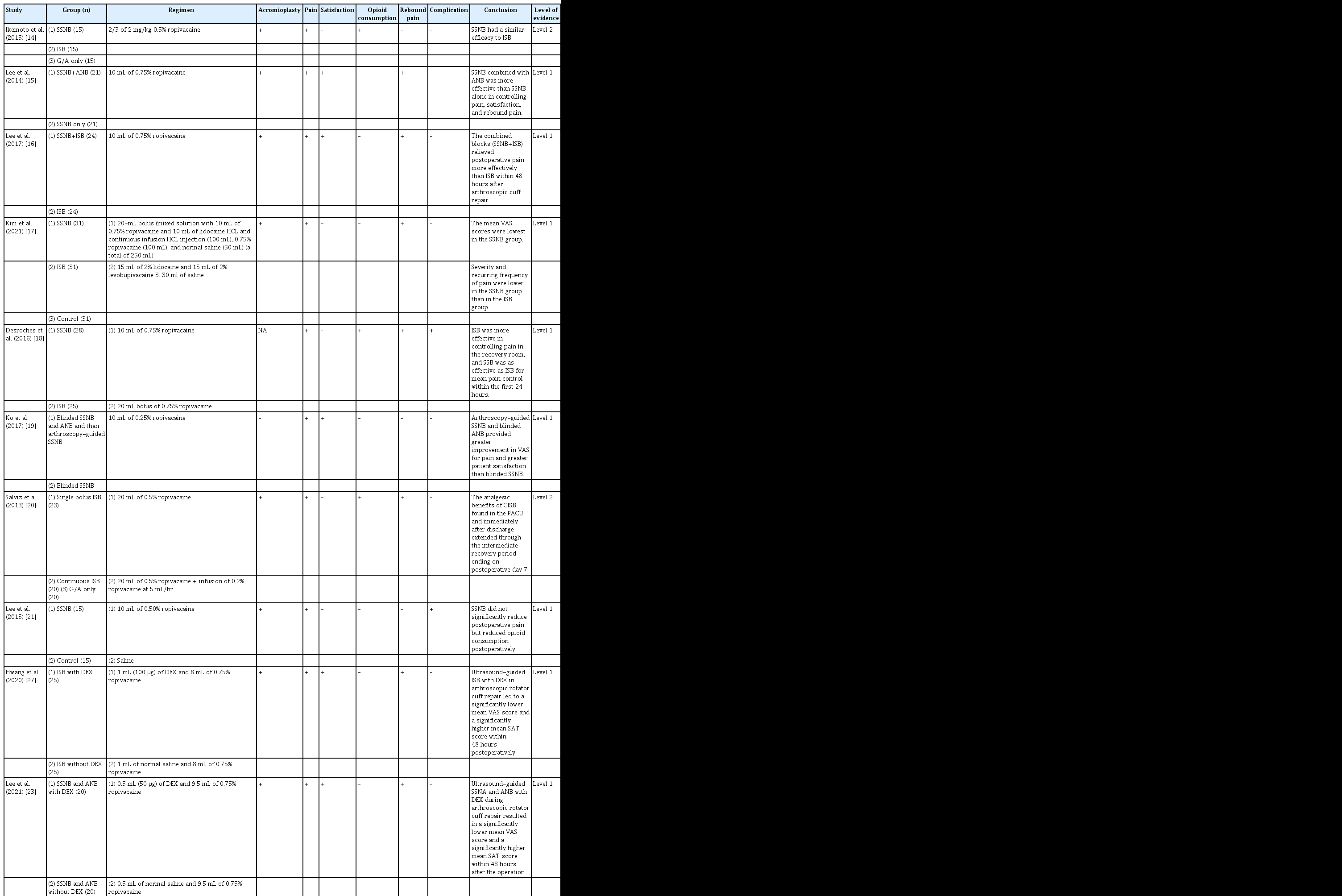
Randomized control trials that analyzed the effects of regional blocks in arthroscopic rotator cuff repair
ANATOMY OF SHOULDER SENSORY NERVE
The posterior cord for the brachial plexus innervates the glenohumeral joint, and there are three peripheral nerves that innervate the capsule: the suprascapular nerve, axillary nerve, and lateral pectoral nerve [25]. Some studies have shown that these nerves have articular branches [26,27].
REGIONAL BLOCKS
Interscalene Brachial Plexus Block
The ISB has been increasing in shoulder arthroscopic surgery because it effectively reduces postoperative pain and use of opioids [5]. The ISB can be applied as a single bolus blockade or a continuous infusion using an indwelling catheter [28]. A single bolus ISB can provide 8 hours of analgesic effect after an operation, and a continuous infusion reduces pain for up to 2 days postoperative [29,30]. The ISB induces less oxidative stress during surgery and can be helpful for perioperative hemodynamic stability [31]. Salviz et al. [20] compared outpatient ARCR patients given a single bolus ISB, a continuous infusion ISB, or general anesthesia. Patients with continuous infusion ISB had less pain and used fewer narcotics than others. Abdallah et al. [29] analyzed 23 randomized controlled trials including 1,090 patients and concluded that single-bolus ISB could provide effective analgesia 8 hours after shoulder surgery. However, after 24 hours, some patients reported rebound pain and showed no difference in pain compared to patients who did not receive the ISB. Kim et al. [32] analyzed 117 patients who underwent ARCR and divided them into three groups (single bolus, continuous infusion, and general anesthesia). They demonstrated that, in the single bolus group, the mean visual analog scale (VAS) score changed from 0.85 to 4.93 between 1 and 12 hours after ARCR, and the use of narcotics in that group showed no difference compared with the other groups. They also reported that the ISB provided immediate pain control until 6 hours after surgery, with a significant rebound effect at 12 hours postoperative. Malik et al. [24] reported that continuous infusion was useful, but about 30% of patients experienced catheter failure, and the risk of phrenic nerve palsy and permanent neuropathy was higher than for a single bolus.
Yun et al. [33] reported that continuous-infusion ISB was more effective than a single bolus of ISB with intravenous PCA. Another study found that the failure rate of ISB was 13%, and one-third of the patients required intravenous pain medication [34]. However, Singh et al. [35] reported that ultrasound-assisted ISB was ultimately successful in almost all cases (99.6% of 1,319 patients), and 99.06% of patients responded that they were satisfied.
Suprascapular Nerve Block and Axillary Nerve Block
Recently, SSNB and ANB have been suggested to reduce postoperative pain after ARCR. These blocks can provide safe and effective intra- and postoperative analgesia during arthroscopy. Nam et al. [36] studied the anatomical location of the suprascapular nerve and axillary nerve in a cadaver. The suprascapular nerve is located in the middle of the anterior tip of the acromion and the superior angle of the scapula and at two-fifths of the way from the anterior tip of the acromion to the medial border of the spine. The depth of the suprascapular nerve is 3.2 cm from the skin. The axillary nerve is located three-fifths of the way from the acromial angle to the inferior insertion of the teres major muscle. The depth of the axillary nerve is 2.1 cm from the skin. Lee et al. [15] showed that ultrasound-guided ANB combined with SSNB in ARCR had better outcomes in mean VAS in the first 24 hours after ARCR than with SSNB alone. Zhao et al. [37] also reported that SSNB and ANB had a better analgesic effect and greater patient satisfaction than SSNB alone. George et al. found that SSNB and ANB reduced opioid consumption after ARCR [38]. Barber [39] showed that SSNB could allow a patient to be discharged earlier from the hospital. Kim et al. [17] reported that arthroscopy-assisted SSNB is not inferior to ultrasound-guided continuous ISB for postoperative pain control and has few neurologic complications. Hussain et al. [40] conducted meta-analysis of SSNB versus ISB. They showed that there was no difference between SSNB and ISB in postoperative opioid consumption and, in the immediate postoperative recovery room, ISB reduced pain better than SSNB. However, at other times, there was no difference. Also, SSNB had fewer side effects [40]. Another meta-analysis showed that SSNB had a higher mean VAS than ISB at rest and while moving. Also, SSNB had a lower rate of complications such as Horner syndrome, numbness, dyspnea, and hoarseness. The suprascapular nerve is anatomically far from the phrenic nerve, but the axillary nerve is close to the phrenic nerve [41]. The ANB may affect the phrenic nerve, which could bring about diaphragmatic palsy and respiratory problems. Hand numbness and weakness, which are side effects of ISB, are less common with SSNB [42]. SSNB and ANB can be performed blind, arthroscopy-assisted, or ultrasound-assisted. Taskaynatan et al. [43] found that the success (including semi-success) rate of ultrasound-assisted SSNB assessed with neurostimulation was 21 of 27 (5 were successful, 16 were semi-successful). Ultrasonography is a radiation-free and real-time tool for verifying the location of the needle tip around the suprascapular notch for the suprascapular nerve and the posterior circumflex humeral artery for the axillary nerve. Ultrasound-assisted block is more effective than a blinded block [44,45]. Lee et al. [21] and Ko et al. [19] found that arthroscopy-assisted block was highly effective in controlling postoperative pain. Furthermore, Lee et al. [16] reported that arthroscopy-guided SSNB combined with ISB resulted in lower mean VAS and higher patient satisfaction scores than ISB alone. In their study, the authors found that the difference in duration between the two blocks might have led to a “fade away effect,” a delay in mean timing of the rebound pain, decreasing the number of patients who experienced rebound pain in the group treated with SSNB combined with ISB compared to the group who received ISB alone.
Combined Use of α2-Agonist
Dexmedetomidine (DEX), a selective agonist of α2-adrenergic receptors, can be an effective adjuvant to local anesthetics for peripheral nerve blocks [22,23]. Preclinical and clinical studies have described a prolonged duration of analgesia when DEX was added to ropivacaine for regional nerve blocks [22,23]. One clinical trial found that ultrasound-guided ISB with DEX in ARCR led to a significantly lower mean VAS score and a significantly higher mean patient satisfaction score within 48 hours postoperatively, showing lower mean interleukin (IL)-6 and IL-8 levels than ISB alone with delayed rebound pain [22]. Another clinical trial reported that SSNB and ANB with DEX led to a similar effect as ISB with DEX. Additionally, SSNB and ANB with DEX resulted in later mean timing of rebound pain accompanied by significant changes in IL-8, IL-1β, and serotonin levels within 48 hours after the operation [23].
DISCUSSION
The most important finding of this review was that SSNB and ANB are not superior to ISB in reducing postoperative pain after ARCR. In addition, there was no difference in postoperative opioid consumption. Also, SSNB and ANB had fewer side effects than ISB. Pain control after ARCR is an issue of constant interest. The ARCR is considered one of the most painful arthroscopic shoulder surgeries, so postoperative pain control is important for early rehabilitation and recovery. There are many methods used for pain control, including PCA, opioids, and regional blocks. Regional blocks such as ISB and SSNB have recently been approved for pain control after shoulder arthroscopy. Koga et al. [46] showed no significant differences between SSNB and ISB regarding the use of additional analgesia, such as intravenous PCA and diclofenac. Sun et al. [47] reviewed a meta-analysis of randomized controlled trials and reported that the SSNB group experienced less pain control in the post-anesthesia care unit than the ISB group but experienced the same or higher pain control at later times. And SSNB with ANB could provide better pain control than SSNB alone [37]. This could be explained that the suprascapular nerve has a few cutaneous innervations so SSNB cannot influence skin incision and the suprascapular nerve innervates only 70% of joint capsule [48] and the axillary nerve innervates 25% of the joint capsule [26]. However, SSNB with ANB is not superior to ISB [40]. Opioids are commonly used for pain control after shoulder surgery, but they have side effects such as vomiting, nausea, respiratory depression, and low blood pressure [49]. All three block types can reduce opioid consumption [20,38]. but there are no differences in opioid use between ISB and SSNB [17,47]. The rebound effect, which manifests as increased pain after a period of time, is found for both SSNB and ISB, especially 10 hours postoperatively [50]. However, another study reported that SSNB with ANB decreased the rebound effect compared to SSNB alone [15]. In this study, the difference in duration between the two blocks might lead to a “soft landing effect,” which could decrease rebound pain with ANB combined with SSNB compared to SSNB alone. As we mentioned, there can be block-related complications after ISB, such as diaphragmatic hemiparesis, pneumothorax, or respiratory distress [51]. Some studies found that SSNB brought about lower incidence of those complications. Although ISB provides higher pain control in the immediate postoperative period, patients at risk of pulmonary problems should receive only ISB. The SSNB can be a safer choice in patients with chronic obstructive pulmonary disease [52], obstructive sleep apnea [53], and obesity [54]. The SSNB is relatively easier and faster to apply and is also safer with lower complication rates [46].
CONCLUSION
The ISB, SSNB, and ANB are commonly used for relieving perioperative pain from ARCR. There is no difference between ISB and SSNB in pain control or opioid consumption. The SSNB has a lower complication rate and can be more easily applied than ISB. Combined regional blocks might have a synergistic effect in relieving rebound pain, and DEX tends to improve the effect of regional blocks with an alteration of pain-related cytokines. While SSNB and ANB are easily performed by experienced orthopedic surgeons, ISB and DEX should be performed with cooperation of an anesthesiologist, considering the possible complications. Adequate regional blocks can be helpful for postoperative pain control of ARCR within 48 hours after surgery.
Notes
Financial support
None.
Conflict of interest
None.