During growth, numerous secondary ossification centers appear in the cartilaginous apophyses and epiphyses of the shoulder, which eventually fuse with the primary ossification centers to form the bony components of the mature shoulder. In parallel, several changes in growth plate morphology occur in a predictable, chronological manner [1,2].
Normal development of secondary ossification centers in the growing shoulder and changes in growth plates may make distinguishing between normal and pathologic images challenging [3-5]. In pediatric patients who sustain shoulder trauma with clinical suspicion of a fracture, plain radiography is the first examination performed in the emergency department. However, interpreting these images is not straightforward, and is even more difficult for clinicians who are not trained in pediatric specialties. This can lead to the use of advanced emergency imaging techniques such as computed tomography (CT), with increased costs and radiation-related risks for the patient. Familiarity with the approximate age at which ossification centers develop as well as sex differences, location, appearance, and fusion of these centers is crucial to accurately interpret imaging studies in a child or adolescent following shoulder trauma.
The purpose of the present report is to analyze a case in which confusion in the interpretation of normal glenoid anatomy in a skeletally immature patient following trauma caused a misdiagnosis of fracture, leading to consideration of surgical treatment. Alternative diagnostic methods are presented, and a review of the normal ossification and fusion of the secondary centers and growth plates of the glenoid during development is provided.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was obtained from the patient's family prior to submission. This study was conducted in accordance with the principles of the Declaration of Helsinki.
CASE REPORT
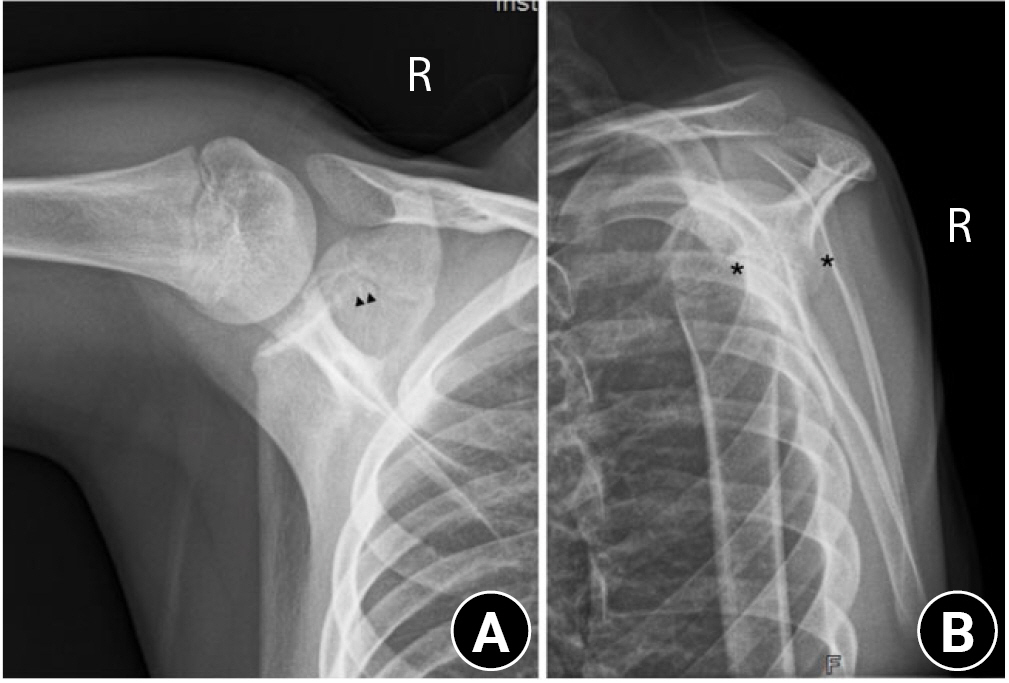
A male adolescent, aged 13 years and 6 months, was referred to our center for pediatric orthopedic care for potential surgical treatment following a diagnosis of intraarticular glenoid fracture. The patient had sustained direct trauma to the right shoulder after falling from a height of 1 meter while playing basketball. Initial X-rays (Fig. 1) and CT images from the referring center were provided on a compact disc; these tests were initially requested at the center of origin due to suspicion of glenoid fracture (Fig. 2) and were originally interpreted as follows: âFracture line running parallel to the glenoid surface and extending to the ossification nucleus of the coracoid, with minimal anterior displacement of a 3-mm-thick bone fragment, measuring 16 mm in the anteroposterior and 14 mm in the craniocaudal axis. The fracture line appears to be fused to the rest of the scapula at its superior margin. A slight irregularity of the glenoid surface is also identified at the inferior margin with 2 millimetric bone fragments. Slight widening of the glenohumeral joint related to joint effusion. There are no other alterations.â
On evaluation by a pediatric orthopedic specialist, the patient had mild swelling and mild pain on palpation of the posterior area of the scapula, though no pain in the clavicle or humeral head. Mobility was limited to 160Âș of forward elevation and 140Âș of abduction; rotation was preserved but mildly painful. Results of distal neurovascular examination were normal. After clinical evaluation and review of the imaging tests performed at the center of origin, radiographs of the contralateral shoulder were obtained (Fig. 3), which closely resembled the injured shoulder. Co-evaluation of CT images alongside a pediatric musculoskeletal radiologist ruled out the presence of a right glenoid fracture. The patient was immobilized with a sling and an elective magnetic resonance imaging (MRI) scan was ordered to confirm the absence of glenoid fracture.
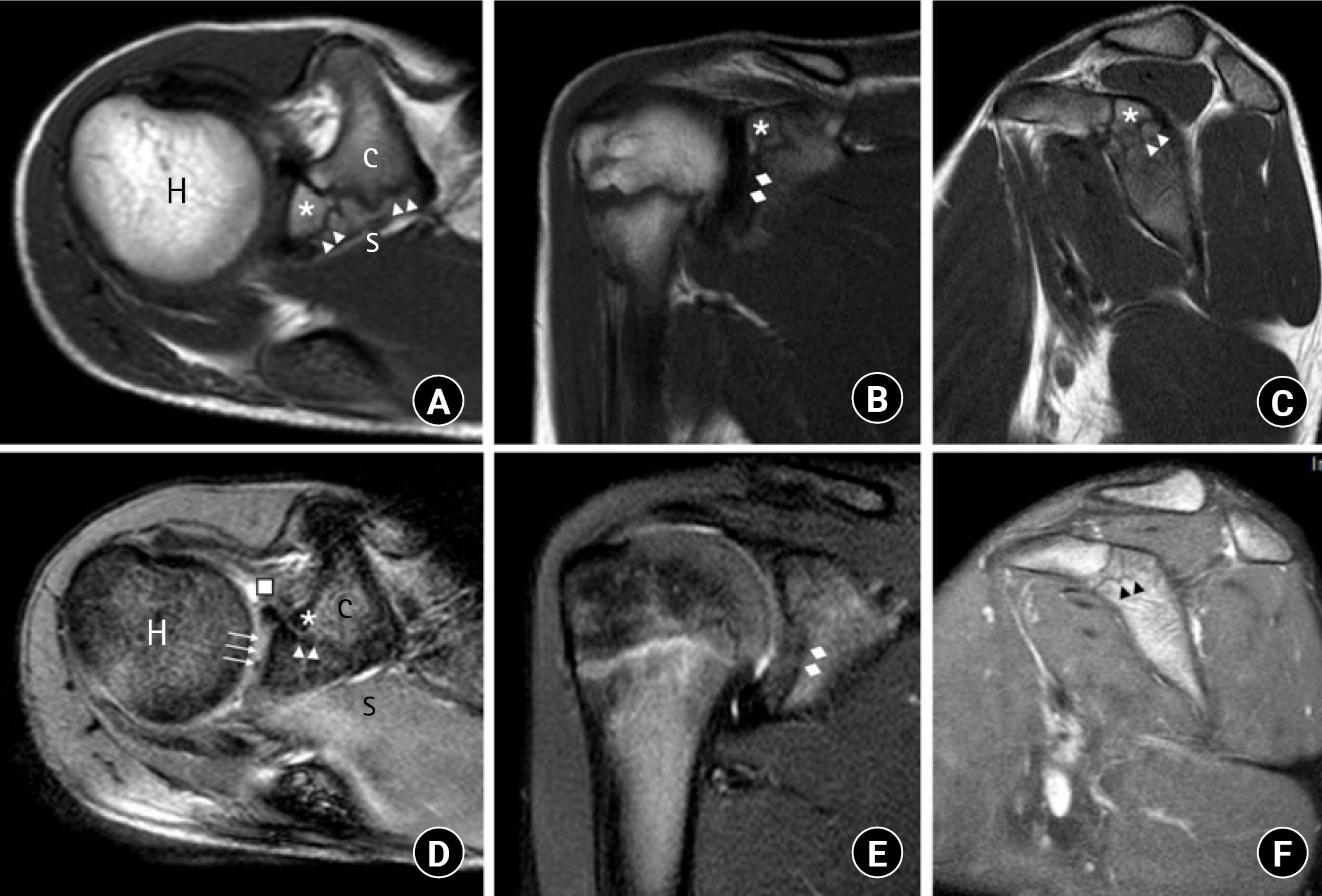
MRI of the right shoulder is presented in Fig. 4. The absence of glenoid fracture was confirmed based on the normal ossification pattern of the glenoid in the absence of other noteworthy findings in the context of trauma, such as bone and soft tissue edema. Clinically, the patient showed an uneventful course, with resolution of pain and recovery of full range of motion and strength at one week.
DISCUSSION
The increasing popularity of competitive contact sports among children and adolescents places them at greater risk for traumatic shoulder injuries. In addition, the presence of physeal plates in skeletally immature patients makes them more prone to injury overall. Despite this increased exposure to injury due to high-energy trauma, orthopedic surgeons are generally less aware of how to accurately interpret imaging tests of the glenohumeral joint in these age groups, potentially leading to errors and incorrect diagnoses [3-5].
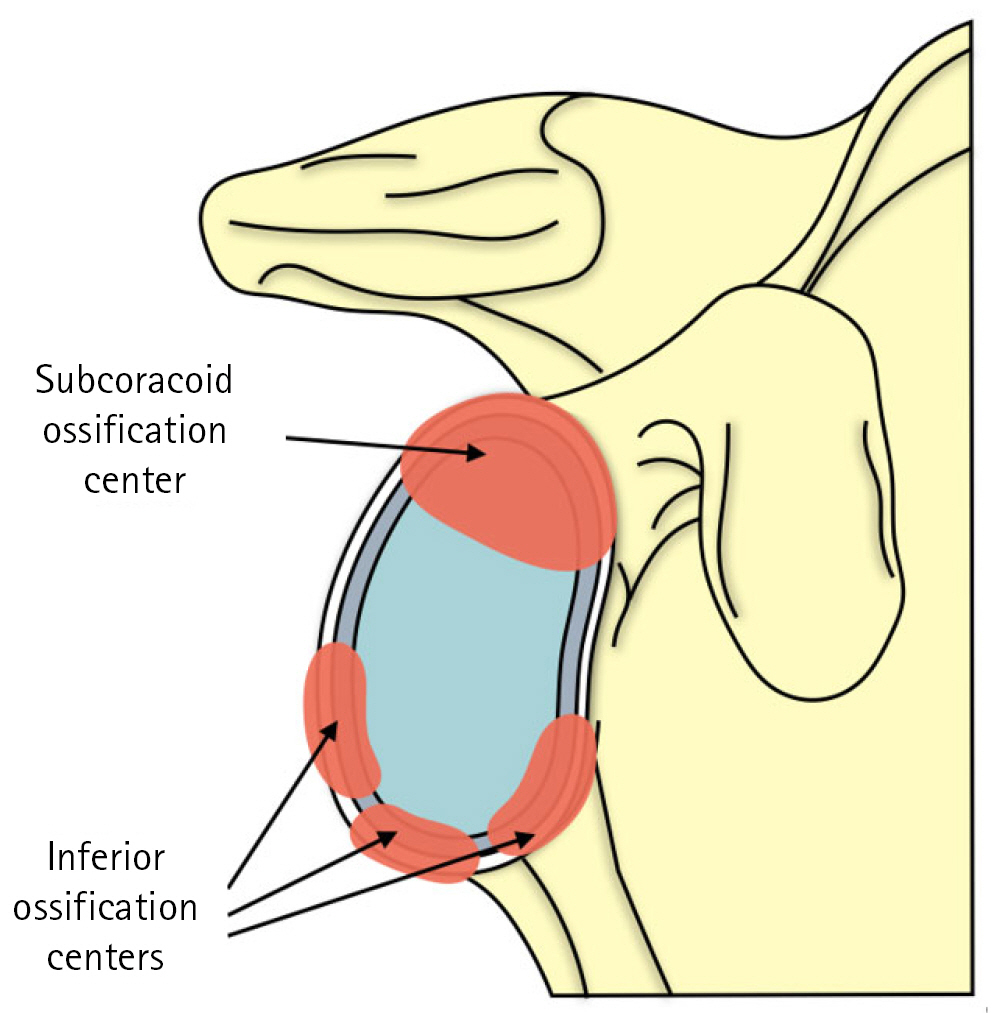
In the present case, normal ossification of the subcoracoid ossification center and the glenoid-coracoid interface was initially confused with a fracture of the superior part of the glenoid extending to the coracoid process. Development of the glenoid and coracoid base in childhood is unique due to the presence of a bipolar growth plate and various secondary ossification centers. In the coracoid-scapular growth plate, endochondral ossification occurs in two directions; closure begins by the age of 13 years and the growth plate is completely fused by age 17 years [1]. The secondary ossification centers comprise two components (Fig. 5):
(1) The subcoracoid ossification center is the first secondary ossification center of the scapula to ossify, forming the upper third of the glenoid articular surface. It usually appears between the ages of 9 and 12 years, and fuses with the body of the scapula between 12 and 16 years of age [1]. The subcoracoid ossification center shares a physis with the base of the coracoid ossification center and can be confused with nondisplaced fractures of the coracoid base [6], as in the present case.
(2) The lower two-thirds of the glenoid articular surface is formed by multiple secondary ossification centers of the inferior glenoid arranged in a horseshoe pattern; these usually appear at around 11 to 14 years of age and fuse between the ages of 12 and 16 years [1]. Recent MRI studies have found that the anteroinferior ossification center may exhibit more delayed ossification and fusion than the rest, which may be a potential confounding factor when analyzing cases of glenohumeral instability and may simulate a Bankart lesion on MRI [1,2].
On routine plain radiographs, the secondary subcoracoid and inferior glenoid ossification centers are not always visible, as in the case presented here. Given the variability of fusion of the secondary ossification centers depending on age and sex and changes in the growth plates, use of the contralateral shoulder radiograph allows reliable comparison to determine the presence of a fracture line or, alternately, a normal growth plate [6,7]. Ossification centers are visible in all planes on CT scan, but most optimally on sagittal and coronal images; these appear as multiple linear foci of bone running parallel to the primary ossification center of the glenoid and should not be confused with osteochondral lesions, as in the initial diagnosis of the present case [4,5]. Interpretation of a fracture with an anterior displacement of a 3-mm-thick bone fragment and the presence of 2 millimetric bone fragments at the inferior margin led the attending physicians at the first health center to incorrectly consider surgery, when these fragments actually corresponded to the normal secondary ossification centers of the glenoid [8].
MRI in the skeletally immature shoulder should include sequences capable of detecting subtle physeal injury, such as three-dimensional fat-suppressed spoiled gradient recalled echo sequences, which help characterize the normal morphology of the glenoid, growth plates, and the developing ossification centers and reliably distinguish them from subtle acute injuries [2]. The sequential glenoid ossification and fusion pattern should be used as a guide when interpreting pediatric MRI scans of the shoulder.
Careful clinical interview and physical examination should guide treatment in cases where pathology must be differentiated from normal developmental variants. Despite the recent increase in shoulder trauma, scapula fractures are extremely rare, especially in the pediatric population, due to the additional protection provided by the periosteum. Furthermore, as in adults, these injuries are associated with very high-energy trauma such as motor vehicle accidents and are frequently associated with severe cranioencephalic, thoracic, axial skeletal, and other upper limb fractures [9]. Likewise, the findings of physical examination of a patient with a glenoid fracture tend to include considerable swelling and functional limitations, which were not observed in the patient described here. Although this patient had limited mobility and pain on palpation, these symptoms were mild and did not suggest a high-energy fracture, but rather simple trauma.
In conclusion, normal sequential patterns of glenoid maturation may simulate a fracture in traumatic settings. Orthopedic surgeons must be familiar with the normal anatomy of the growing shoulder, its secondary ossification centers, and growth plates in order to avoid errors when interpreting imaging tests in the pediatric shoulder. Age, sex, and mechanism of injury can aid in diagnosis. Use of contralateral radiography for comparison and MRI can help differentiate normal developmental changes from pathologic changes in skeletally immature patients and guide the diagnosis and management of pediatric shoulder pathology.