Chronic locked anterior shoulder dislocation with impaction of the humeral head onto the coracoid: a case report
Article information

Abstract
The glenohumeral joint is one of the most commonly dislocated joints. When dislocated, the humeral head typically moves anteriorly and medially within the soft tissues adjacent to the glenoid. We present a case of a 64-year-old female who presented with a locked anterior shoulder dislocation with impaction of the humeral head onto the coracoid. To our knowledge, this is the first reported instance of humeral head impaction onto the coracoid causing the shoulder dislocation to be irreducible by closed means. Complications of this dislocation can include humeral head deformity, pseudoparalysis, brachial plexus injury, and significant pain.
Level of evidence
V.
The glenohumeral joint is the most commonly dislocated large joint in the body, with an incidence rate of 23.9 per 100,000 person-years, and the vast majority of dislocations is anterior [1]. There is a bimodal distribution, with peaks occurring most commonly in young males from high energy trauma and geriatric females from ground-level falls. The standard of care for most shoulder dislocations is closed reduction followed by a brief period of immobilization. Common complication in the young cohort includes recurrent instability, while that in the geriatric cohort includes rotator cuff tear. In a large prospective trauma database study of 3,644 patients who sustained an anterior shoulder dislocation, 1,215 (33.4%) had a rotator cuff tear or a greater tuberosity fracture with associated risk factors including female sex, advanced age, and low-energy fall [2].
In anterior shoulder dislocation, the posterior portion of the humeral head typically collides with the anterior rim of the glenoid resulting in a Hill Sachs lesion. Hovelius et al. [3] found that 54% of anterior shoulder dislocations were associated with Hill Sachs lesions, which can increase the risk of recurrent dislocation. Associated injuries occur in up to 40% of anterior shoulder dislocations and include brachial plexus injury, labral as well as glenoid damage, and humeral head damage [4]. Typically, in an anterior dislocation, the humeral head lies anterior and medial within the soft tissues adjacent to the glenoid. The following is a case report of a chronic locked anterior shoulder dislocation with impaction of the humeral head onto the coracoid, which to our knowledge has yet to be described in the literature.
CASE REPORT
The patient is a 64-year-old female with a history of chronic right shoulder pain and dysfunction. Several months prior to her right shoulder surgery, she was seen by an outside orthopedic surgeon. Based upon documentation, she had limited shoulder range of motion, and magnetic resonance imaging (MRI) demonstrated rotator cuff arthropathy including subscapularis deficiency. Three months prior to being seen, she had experienced a traumatic injury with an anterior shoulder dislocation, which was “reduced” at an outside institution. Since the injury, she had noted worsening shoulder pain and diminished motion.
Per our institution rules, institutional review board approval is not required for a case report. Consent was obtained from the patient and she is aware that her case was being used for publication.
The patient’s past medical history is significant for diabetes mellitus; she was treated with methotrexate for rheumatoid arthritis for the previous 6 months and with rivaroxaban for atrial fibrillation. She works as a farmer. Her physical exam demonstrated pseudoparalysis of the shoulder with intact axillary nerve function. Her preoperative range of motion was forward flexion to 10° (contralateral 150°), abduction 10° (contralateral 150°), external rotation with elbow at side to 0° (contralateral to 15°), and internal rotation to greater trochanter (contralateral side to L3). Shoulder imaging including radiographs and computed tomography (CT) scan demonstrated an anterior dislocation of the glenohumeral articulation with impaction of the humeral head onto the coracoid process (Figs. 1 and 2). For the glenoid, there was central bone wear consistent with Walch classification A1. An MRI scan 10 months prior to surgery demonstrated a high riding humeral head with complete deficiency of the rotator cuff to include the subscapularis with acetabularization of the acromion consistent with Hamada classification 4b (Figs. 3 and 4).

Anterior-posterior radiograph of the right shoulder demonstrating humeral head impaction onto the glenoid.

Axial computed tomography image demonstrating impaction of the humeral head onto the coracoid.

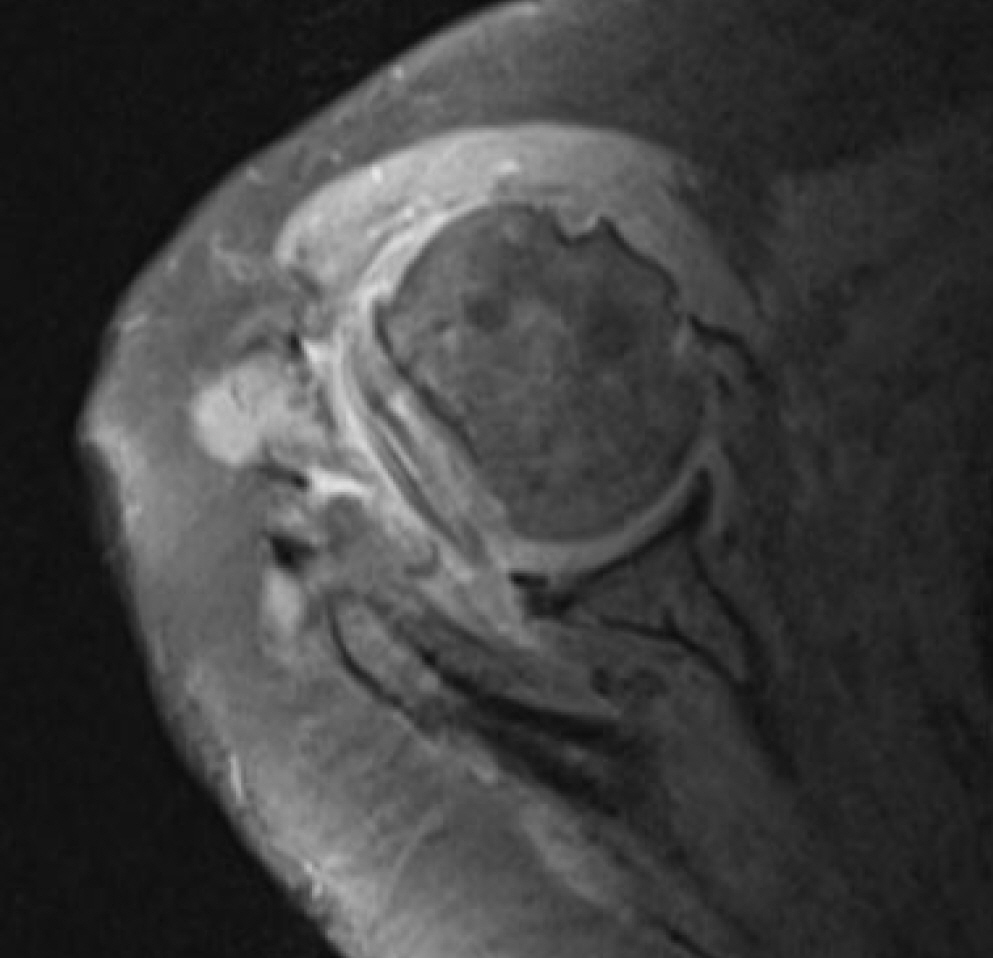
Coronal magnetic resonance imaging showing rotator cuff arthropathy with high riding humeral head.
Axial magnetic resonance imaging demonstrating retracted subscapularis tear.
Giving the patient’s chronic locked anterior shoulder dislocation with impaction of the humeral head onto the coracoid with associated pseudoparalysis, she was indicated for surgery in the form of reverse total shoulder arthroplasty. The implant utilized was the Reverse Shoulder Comprehensive cementless modular system with mini stem (Zimmer-Biomet). The humeral component was placed at 20° of retroversion. The glenoid component had 10° of built-in inferior angulation, and the glenosphere was further offset inferiorly 2.5 mm relative to the baseplate. There was slight baseplate lateralization by reaming to create a bone ridge inferior along the inferior aspect of the glenoid but, not on the superior portion. A standard deltopectoral approach was utilized with extreme caution for medial dissection to protect the musculocutaneous nerve. Her surgery was uneventful including her postoperative rehabilitation. At her near 1-year postoperative follow-up visit, physical examination demonstrated shoulder forward flexion 105°, abduction 85°, and external rotation to neutral (Figs. 5 and 6). Radiographs demonstrated appropriate alignment of the reverse total shoulder prosthesis (Fig. 7).

Clinical image demonstrating the patient’s forward flexion (10 months postoperative).

Clinical image demonstrating the patient’s abduction (10 months postoperative).

Anterior-posterior radiograph demonstrating reverse total shoulder prosthesis (10 months postoperative).
DISCUSSION
The glenohumeral joint is the most commonly dislocated large joint in the body, and over 95% of glenohumeral dislocations are anterior [5]. Defects of the anterior glenoid rim and labrum are common in patients who have multiple anterior glenohumeral dislocations. In 2014, Schneider et al. [6] published a case report in which a 32-year-old man with recurrent anterior glenohumeral dislocations was diagnosed with an avulsion fracture of the coracoid process. He was treated with a Latarjet procedure; 3 months post-surgery, he had a satisfying range of motion without instability or pain. There are no reports in the literature of chronic locked anterior shoulder dislocation with impaction of the humeral head onto the coracoid.
As previously stated, anterior glenohumeral dislocations have a significant risk of associated injuries including bony injury, which increases risk of repeat dislocation and soft tissue injury; for example, to the rotator cuff, as well as to the brachial plexus including the musculocutaneous nerve. When glenohumeral dislocations are untreated and left dislocated for a long period of time, there is significant soft tissue contracture, and the humeral head can become impacted against bony structures such as the anterior rim of the glenoid or the coracoid. In our case, the coracoid created a significant divot in the humeral head (Fig. 8). This impaction led to shoulder dysfunction, loss of motion, and pain.

Intraoperative clinical image demonstrating impaction deformity of the humeral head.
Our patient was treated with reverse total shoulder arthroplasty through a standard deltopectoral approach. The patient had excellent restoration of range of motion and decreased pain. In 2017, Statz et. al. [7] evaluated the role of reverse total shoulder arthroplasty, total shoulder arthroplasty, and hemiarthroplasty for treatment of chronic anterior shoulder dislocation. They found that reverse total shoulder arthroplasty provided greater pain relief and improvement in range of motion compared with total shoulder arthroplasty and hemiarthroplasty.
Our patient’s dislocation occurred in the superomedial direction, likely due to the patient’s pre-exiting massive rotator cuff tear demonstrated on the MRI scan she had undergone several months prior to the present injury. In 2009, Matsuzaki et al. [8] published a case report of an 83-year-old patient with Parkinson disease who had anterosuperior dislocation with deficiencies of both the supraspinatus and subscapularis tendons. This case relates to our patient as our patient also had deficiencies of both the supraspinatus and subscapularis tendons. Deficiencies of these tendons may result in anterosuperior dislocation.
There are several key learning points from this case report. To our knowledge, this is the first described instance of humeral head impaction onto the coracoid, which caused the shoulder dislocation to be irreducible by closed means. This can lead to deformity of the humeral head, pseudoparalysis, and significant pain. Advanced imaging in the form of CT scan or MRI is essential to evaluate alignment of the dislocated humeral head, humeral head and glenoid bone wear/deficiency, and preoperative planning. Last, reverse total shoulder arthroplasty should be considered the standard of care for patients with a chronic locked anterior glenohumeral dislocation.
Notes
Author contributions
Conceptualization: MJO. Project administration: MJO. Writing – original draft: RDL, MJO. Writing – review & editing: RDL, MJO.
Conflict of interest
None.
Funding
None.
Data availability
None.
Acknowledgments
None.