INTRODUCTION
Avascular necrosis (AVN) of the humeral head is a rare complication. Atraumatic AVN of the humeral head is infrequently isolated, coinciding with multifocal osteonecrosis including the hip [1,2]. Following AVN, inflammation, fibrosis, and sclerosis of the humeral head occurs as the body attempts to heal the damaged bone. However, if left untreated, AVN frequently progresses to subchondral fracturing and articular collapse [3,4]. AVN symptoms of the humeral head are commonly unrecognized and non-specific in early stages prior to collapse of the humeral head, often leading to misdiagnosis and inaccurate treatment. Particularly, in a prior study, up to 71% of patients in one cohort had progression of their humeral head AVN in the setting of nonoperative management, highlighting a devastating natural history of the condition [5]. In patients with late-stage AVN, including Cruess stage III–V AVN [6], treatment often requires extensive intervention, including humeral head resurfacing [7,8], hemiarthroplasty [9,10], and total shoulder arthroplasty (TSA) [5,10], because management of the osteonecrosis is unamendable to more conservative measures. In patients with early-stage AVN, including Cruess stages I and II, several measures have been described, most notably core decompression [11-14]. Although core decompression has been well described as a viable option for management of early-stage AVN in the femoral head [15-21], outcome studies related to the humeral head have been relatively limited without complete consensus on superior techniques to optimize patient outcomes and reduce overall AVN progression.
In this article, the etiology, clinical presentation, and classification of AVN of the humeral head, the indications and current techniques for core decompression of the humeral head, and a complete summary of all current clinical outcomes for each core decompression technique, including the use of adjunctive biologics for the humeral head, are presented.
PATHOGENESIS AND ETIOLOGY
Trauma
Traumatic injury of the proximal humerus is the leading cause of AVN of the humeral head. Proximal humerus fractures increase the risk of disrupting both anterior circumflex and posterior circumflex arteries, the primary vascular supply of the proximal humerus. Significant proximal humerus fracture patterns of humeral head AVN have been reported, including 0%–25% risk for three-part fractures [22-24] and 0%–77% risk for four-part fractures [22-25]. The risk of traumatic AVN has a strong correlation with initial medial hinge integrity and length of the metaphyseal head extension [26], and likely associated with displacement-induced stripping of the periosteum and vessels [27]. However, despite the fracture pattern severity, younger age has been associated with greater resistance to AVN [28].
Atraumatic AVN
Although consensus is lacking on the pathogenesis of atraumatic AVN of the humeral head, several theories have been presented. As previously described, AVN develops due to vascular compromise, commonly due to traumatic etiology. However, certain risk factors and genetic predisposition may increase the risk of vascular disruption, increasing the risk for osteonecrosis through increased intraosseous pressure and compromised blood supply [6,29-32]. Although cases can be idiopathic, several risk factors, both direct and indirect, have been proposed, most notably corticosteroid use [33], sickle cell anemia [31,34,35], systemic lupus erythematosus [36], alcohol consumption [37,38], human immunodeficiency virus (HIV) [39-41], and dysbaric osteonecrosis [42,43].
CLINICAL PRESENTATION
AVN of the humeral head is characterized by insidious onset of shoulder pain, often without evidence of an inciting event. Patients can experience significant glenohumeral pain, either at rest or with shoulder motion. Some patients may experience pain at night, limiting sleep. In addition to pain, patients may experience shoulder stiffness or weakness of the rotator cuff. In cases of advanced AVN, there may be clicking/clunking of the shoulder with movement due to either an arthritic or collapsed humeral head. Progressive AVN can lead to intraarticular osteochondral fragments, causing locking or popping. Tenderness with shoulder motion is often delayed to later stages of the disease, with most discomfort occurring with maximum glenohumeral loading at >90° of arm abduction [23].
RADIOLOGIC ASSESSMENT
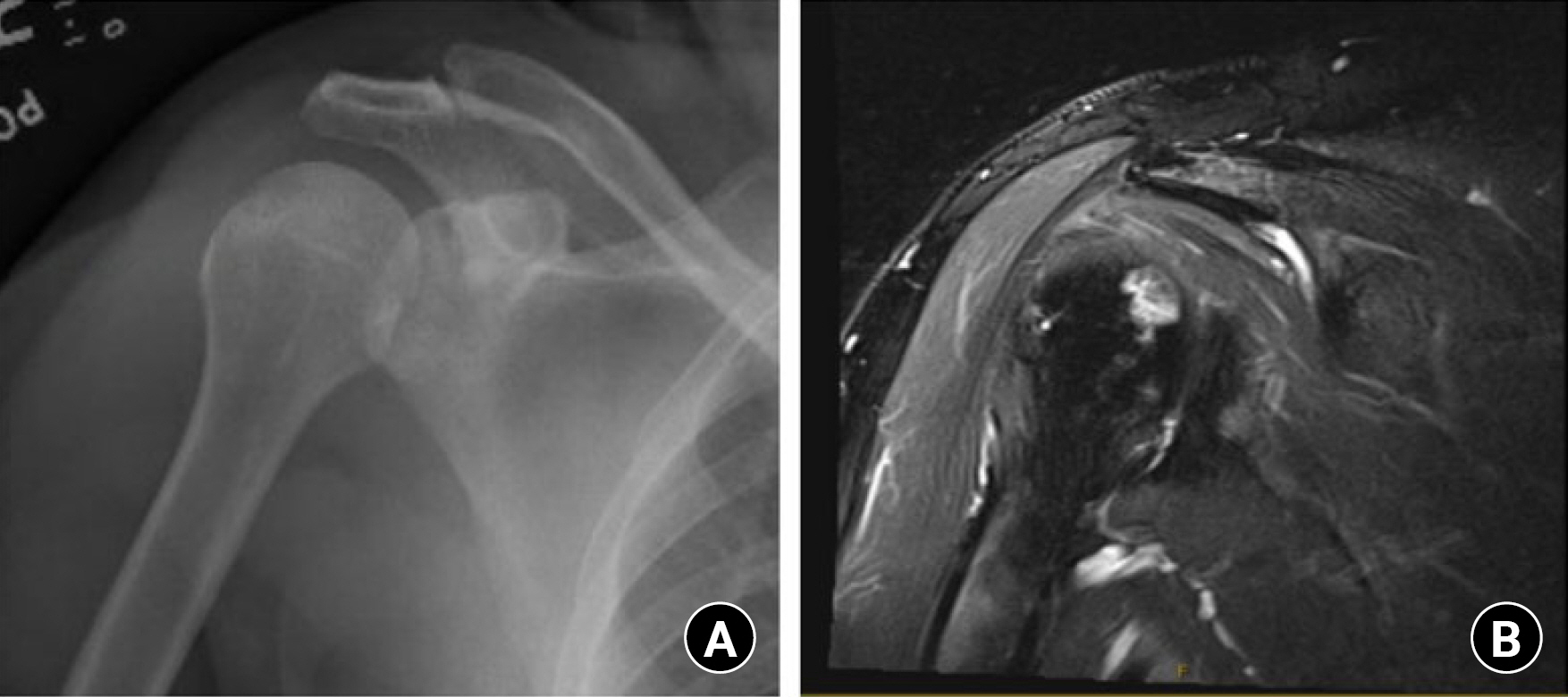
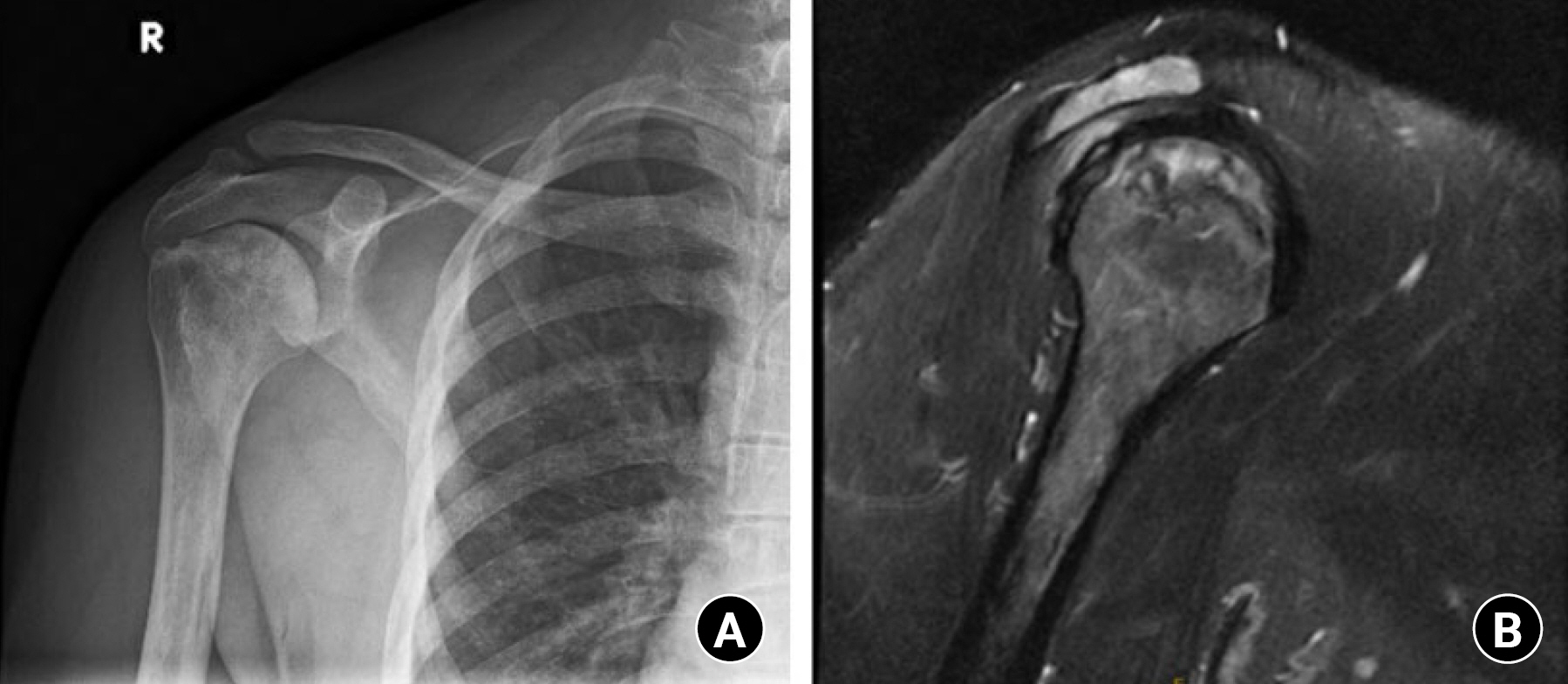
Initial assessment in suspected AVN of the humeral head should include an extensive clinical and radiographic examination to assess for osteosclerosis, subchondral lucency, and frank joint collapse of the humeral head. A history and physical examination for suspected AVN of the humeral head should first be assessed with plain radiography. On plain films, early osteonecrosis of the humeral head is often not detected (Fig. 1). However, signs of sclerosis or cystic changes may be suggestive of underlying AVN (Fig. 2) [44]. With progression of AVN, the articular surface of the humeral head may collapse due to subchondral fracturing in the area of bone necrosis and identified on plain radiographs by the “crescent sign,” an area of subchondral lucency and incongruency of the articular surface. Later stages of AVN progress to flattening, collapse, and progressive degenerative changes [6].
After plain radiography, magnetic resonance imaging (MRI) is considered the modality of choice for the diagnosis of early-stage AVN. The benefits of MRI are associated with sensitive identification of early changes of water and fat content of the bone marrow not evident on plain radiographs [23]. Thus, in cases of suspected osteonecrosis with negative results on plain radiography, MRI of the shoulder should be performed. However, in late stages of AVN, plain radiography and occasionally computed topography (CT) imaging are recommended for further evaluation of subchondral fracturing [23].
CLASSIFICATION
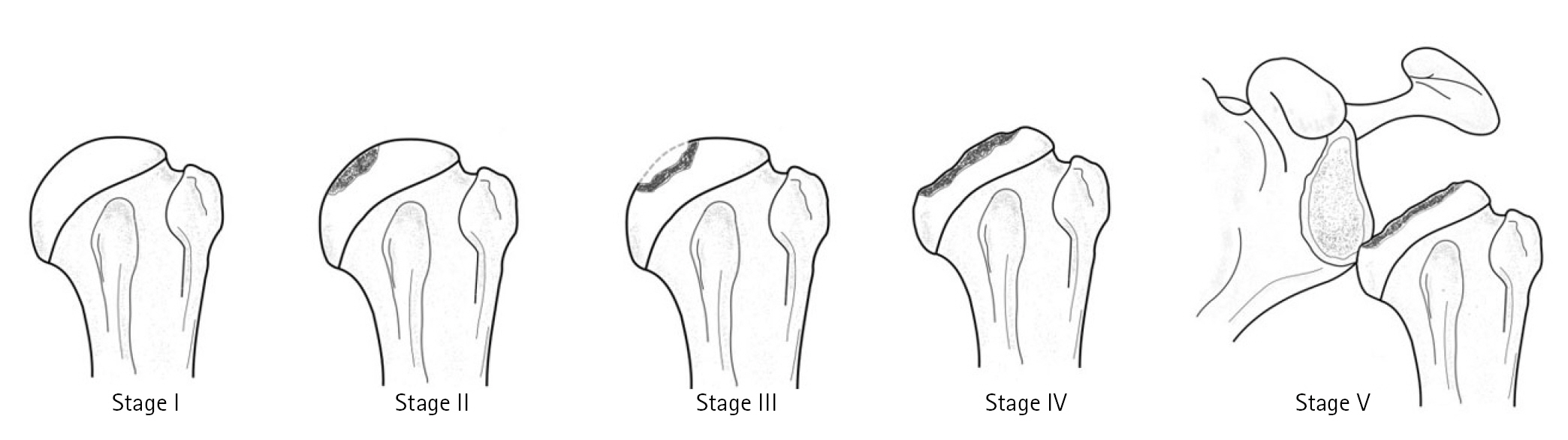
AVN of the humeral head is most commonly classified according to the Cruess staging for osteonecrosis of the humeral head [6] as modified from the Ficat and Arlet classification of the hip [45]. In brief, the Cruess classification describes the severity of osteonecrosis of the humeral head as follows: stage I, negative findings on plain radiographs and bone marrow signal changes on MRI; stage II, plain radiographs showing focal subchondral osteolysis and/or mottled or wedged sclerosis of the superior humeral head without articular collapse; stage III, subchondral collapse and loss of humeral head sphericity, commonly associated with the “crescent sign”; stage IV, extensive subchondral bone collapse and loss of humeral head sphericity and secondary arthritic changes; stage V, progressive osteonecrosis with arthritic changes extending onto the glenoid articular surface (Fig. 3) [11]. In general, the criteria for early (stage I or II) versus late (stage III–V) stage AVN of the humeral head depends on the radiographic and clinical presence of humeral head subchondral collapse in late-stage AVN [11].
NONOPERATIVE MANAGEMENT
In the setting of early-stage osteonecrosis of the humeral head, including stages I and II osteonecrosis where subchondral collapse of the humeral head has not yet occurred, nonoperative management can be explored to address shoulder pain and mechanical symptoms. Prior to considering core decompression or other operative measures, management can include shoulder physical therapy for strengthening and improving range of motion, activity modification, and medical management of any underlying medical conditions that may have contributed to the development of the osteonecrosis as aforementioned. Anti-inflammatory medications may be useful for pain control. However, as previously mentioned, a high rate of progression of humeral head osteonecrosis has been emphasized in prior studies, with more than 71% of patients in mid to late stages having disease progression as early as the 2-year follow-up [5]. This reaffirms the necessity for early diagnosis and intervention to prevent further progression to later-stage AVN, including progression to subchondral collapse and further development of AVN-associated glenohumeral arthritis.
CORE DECOMPRESSION INDICATIONS
Since the introduction of core decompression by Mont et al. [13] for the treatment of the humeral head osteonecrosis, the method has been considered a viable conservative option to prevent further progression of AVN and prolong the time before extensive treatment measures, including humeral head resurfacing, hemiarthroplasty, and TSA, are performed. Although initially described for all stages of humeral head AVN, poor clinical outcomes for patients with late-stage AVN of the humeral head, primarily in Cruess stages IV and V, have been shown in clinical studies. In particular, excellent outcomes in ≥ 88% of patients with Cruess stage I or II AVN of the humeral head were reported in early studies, however, in studies by LaPorte et al. [12] and Mont et al. [36], excellent outcomes in stage III osteonecrosis were observed in only 70% of patients. Additional decline in success rates was observed in stage IV AVN, with excellent outcomes as low as 14% [12]. Furthermore, studies by L'Insalata et al. [5] described five shoulders with stage III AVN that progressed to TSA (80%) or stage IV AVN (20%). Thus, based on early evidence, whether core decompression in stage III AVN produces long-term clinical benefit is unclear because subchondral collapse has already occurred. Nevertheless, core decompression is indicated in symptomatic patients with Cruess stage I or II AVN, however, alternatives to core decompression may be considered in stages III–V depending on patient age, functional status, and consideration of arthroplasty longevity. To date, there have not been sufficient clinical studies to further clarify outcomes of core decompression of the humeral head based on other patient characteristics or preoperative shoulder patient reported outcome scores, limiting selection based on clinically symptomatic patients with radiographic signs of early-stage AVN. However, in general, core decompression should be performed in patients with early-stage AVN of the humeral head without articular collapse (Cruess stages I and II), and in patients in whom nonoperative measures including analgesics, physical therapy, and corticosteroid injections failed [44]. Several techniques have been developed for core decompression of the humeral head, and are described in detail in the following section.
CORE DECOMPRESSION TECHNIQUES AND OUTCOMES
A summary of available core decompression techniques and clinical outcome studies for the humeral head is presented in Table 1.
Anesthesia and patient positioning
Each technique for core decompression is performed under general anesthesia with the patient either in the supine or beach chair position on a standard operating table.
Open technique
Mont et al. [13] were the first to present core decompression for AVN of the humeral head using a standard technique with a 5-mm coring device (single large trephine).The standard open technique involves utilizing the deltopectoral interval. To perform the open technique, a 2-cm incision is made superior to the pectoralis major tendon anterior to the axillary fold. The deltopectoral interval is developed by blunt dissection until the proximal humerus is reached. Care should be taken to not disrupt the common neurovascular structures within the interval [50]. A single coring device is then utilized and drilled into the proximal humeral metaphysis slightly lateral to the bicipital groove. Accurate decompression should be confirmed with intraoperative fluoroscopy corresponding to the lesion position observed on preoperative imaging. Although originally described with a 5 mm trephine, several other techniques have been developed with single trephines ranging from 6 mm–10 mm in size [12,13,36].
Outcomes of open technique
Mont et al. [13] reported good to excellent University of California Los Angeles (UCLA) shoulder score outcomes for core decompression of Ficat and Arlet [45] stage I or stage II humeral head AVN with no progression to TSA. Conversely, 3 of 10 stage III and 5 of 6 stage IV shoulders progressed to TSA, with the 1 stage IV shoulder not progressing to TSA having an outcome of only good. Similar results were observed in follow-up studies by LaPorte et al. [12] and Mont et al. [36], with excellent outcomes of early-stage humeral head AVN and high failure rates in shoulders with stage III–V AVN. This was consistent with studies by L'Insalata et al. [5] in which all five shoulders with stage III AVN progressed to TSA (80%) or stage IV AVN (20%).
Percutaneous technique
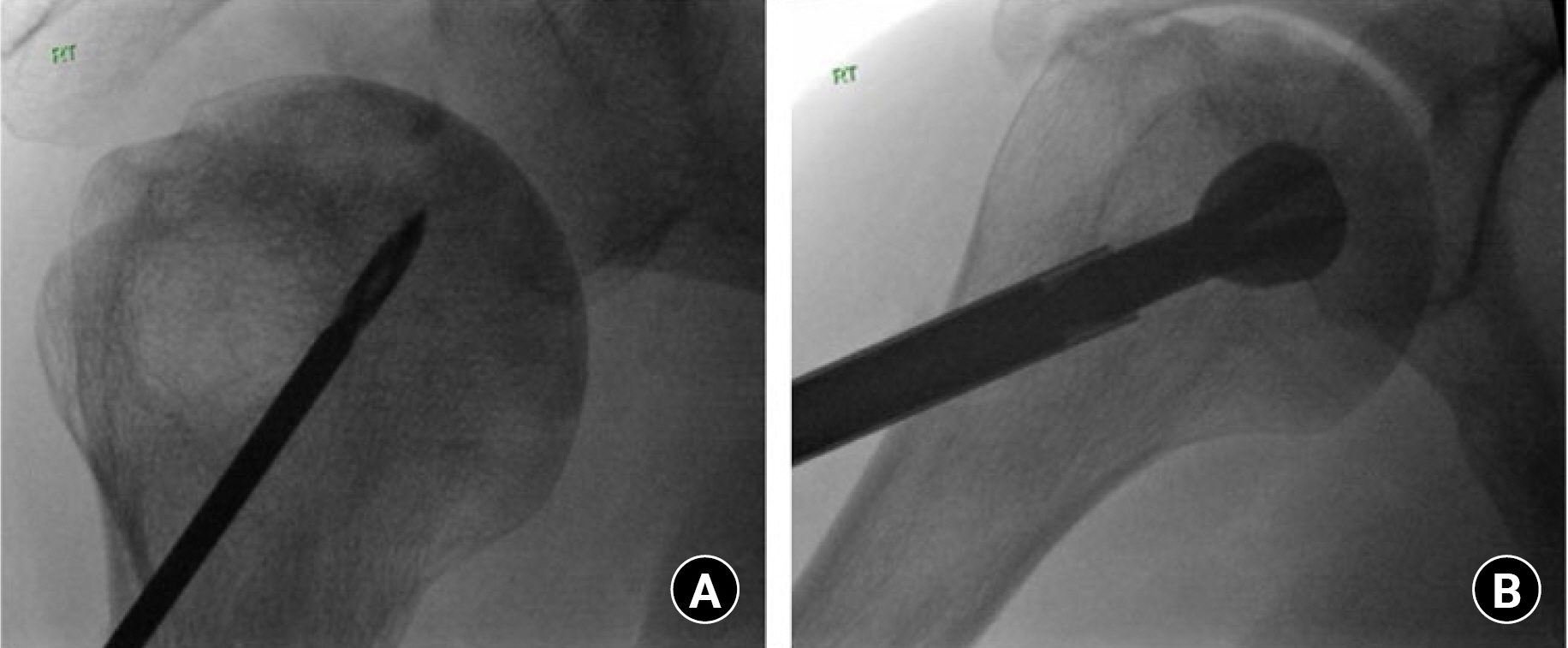
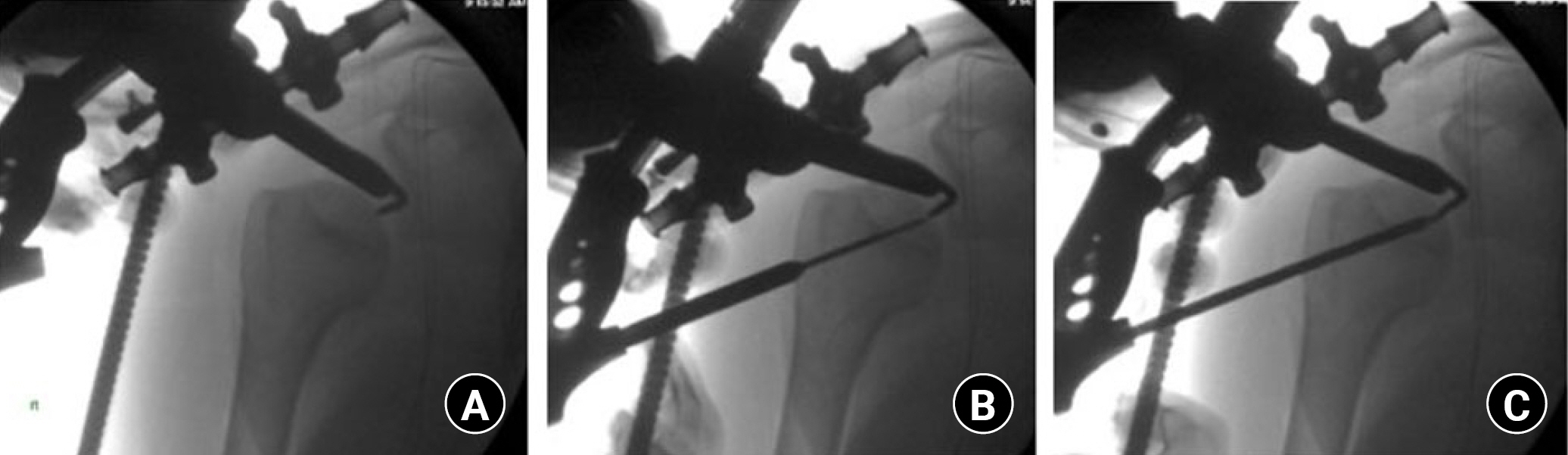
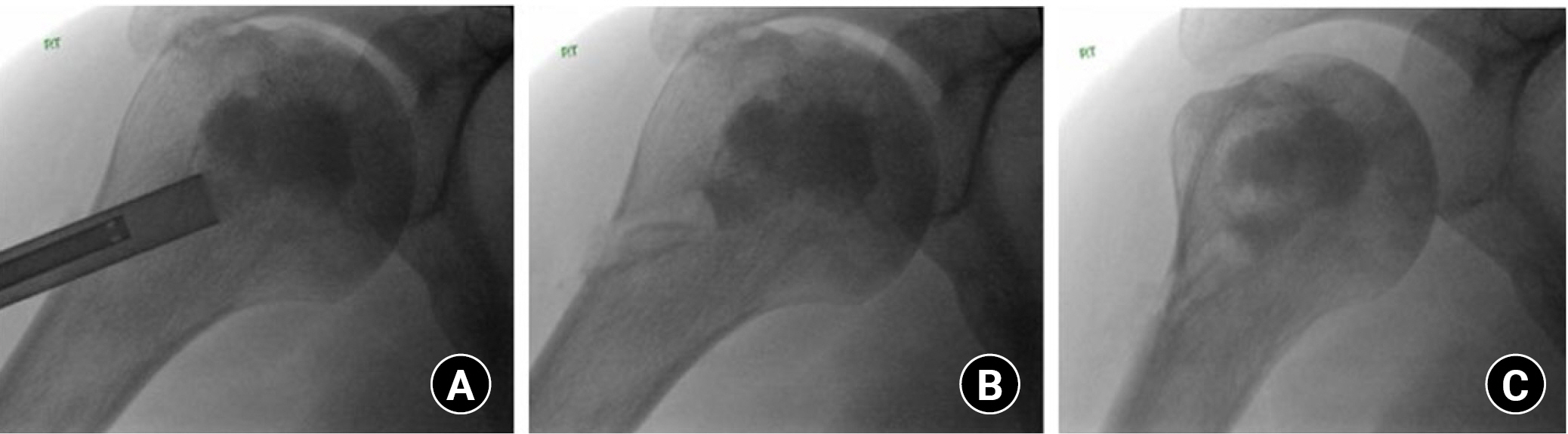
Although the traditional technique for core decompression has been shown an effective technique for both the hip and humeral head, a small-diameter percutaneous technique showed excellent results for core decompression of the hip [16,51]. The inception of this technique was based on the theory that multiple passes into the necrotic lesion will increase the coverage of the necrotic lesion, and the percutaneous technique reduces surgical morbidity in comparison with the larger surgical incisions required for a large trephine. More recently, the technique has been adapted for the humeral head [11]. In brief, the technique by Harreld et al. [11] utilizes multiple small diameter percutaneous perforations using a 3.2-mm Steinmann pin advanced twice, for smaller lesions, or three times for larger lesions, to the epiphyseal lesion under fluoroscopic guidance (Fig. 4). Insertion of the Steinmann pin should be localized lateral to the bicipital groove, reducing risk of damage to the ascending branch of the anterior humeral circumflex artery [52]. Kennon et al. [10] also presented this technique utilizing a standard 2.7-mm drill bit passed several times into the necrotic lesion under fluoroscopic guidance. Although a small-diameter drill is more commonly used, a single large trephine may also be utilized for the percutaneous technique albeit with a larger initial incision to accommodate the larger drill (Fig. 5). The authors recommend a lateral approach when a larger drill, reamer, or trephine is used. Under fluoroscopy, a lateral point of entry inferior to the level of the axillary nerve is localized using a spinal needle. An incision is then made and a blunt dissection performed down to the lateral cortex of the proximal humerus. A blunt trocar can then be used for dilation of the incision and to reduce risk of iatrogenic nerve injury. Next, a standard core decompression with a large trephine is performed as previously described.
Outcomes of percutaneous technique
Harreld et al. [11] assessed the outcomes of patients with Cruess stage I or stage II AVN of the humeral head treated with percutaneous core decompression. In a cohort of 15 patients (26 shoulders), the mean UCLA shoulder scores increased from 14 (range, 10–22) preoperatively to 27 (range, 14–30) postoperatively at the mean follow-up of 32 months (range, 24–41 months). Only 1 patient had poor outcome with a UCLA score of 11 preoperatively and 14 postoperatively, however, this patient was complicated by spondyloarthropathy and multiple joint involvement of the AVN.
Although good outcomes for core decompression were observed in previous studies, mixed results were reported in a case series by Kennon et al. [10] in which 11 patients (11 shoulders) with stage I or stage II humeral head AVN were assessed for outcomes following core decompression. The procedure was performed using a standard 2.7-mm drill bit with multiple fluoroscopically guided passes with concurrent intraoperative ultrasound bone stimulation. Among the 11 patients, 3 were lost to 1-year follow-up. However, two of three patients continued to have persistent pain postoperatively. At the mean follow-up of 17.4 months, seven of the eight remaining patients progressed to further collapse and five required additional resurfacing procedures due to continued postoperative symptoms. Functional outcomes in that study were only assessed following resurfacing, TSA, or reverse TSA, however, the high failure rate and progression within 2 years postoperatively raises concerns for long-term durability of the procedure.
Arthroscopic-assisted technique
The use of arthroscopy in core decompression of the humeral head was first introduced by Chapman et al. [53] as an adjunctive measure for accurate articular assessment and placement of the guide pin. The main premise of this technique is to reduce the risk of iatrogenic perforation of the articular surface while additionally allowing the surgeon to treat coinciding shoulder pathology, including synovitis and chondral pathology, which may limit optimal postoperative recovery. Furthermore, arthroscopy provides the benefit of direct observation of articular surface collapse without the need of an open incision. In brief, arthroscopic-assisted core decompression is performed using two standard portals, including posterior and anterior portals. After the arthroscope is placed in the posterior portal, a standard diagnostic arthroscopy is performed with full assessment of the intraarticular cartilage, labrum, rotator cuff, biceps, and subacromial bursa. During the arthroscopy, any intraarticular pathology should be appropriately managed. In addition, arthroscopy allows for the absence of humeral head collapse, which would contraindicate core decompression, to be confirmed. Once diagnostic arthroscopy is complete, a lateral portal is established and a standard percutaneous core decompression is completed. Intraoperatively, the arthroscope is maintained within the posterior portal to confirm the drill has not disrupted the articular surface of the humeral head.
In addition, the use of an anterior cruciate ligament (ACL) tibial drill guide has been described an effective tool for accurate triangulation of the humeral head AVN lesion while reducing the risk of unnecessary drilling [46,49]. Dines et al. [46] described the technique in terms of a standard arthroscopic-assisted core decompression with use of only the anterior and posterior arthroscopic portals, however, the authors prefer a laterally directed mini-open incision for placement of the ACL targeting guide (Fig. 6). Due to the proximity of the axillary nerve in this anatomic area, the incision should be carefully extended down to the lateral cortex of the humerus. Fluoroscopic imaging is used to localize the necrotic lesion and the ACL tibial drill guide is positioned to triangulate the area of necrosis. Next, a soft tissue protector is placed within the incision and a guide pin is drilled into the lesion. Direct visualization using arthroscopy and fluoroscopy is performed to confirm the lesion has been reached and the pin has not penetrated through the subchondral bone into the cartilage. Then, using a 4-mm cannulated drill, a decompression channel is created by aligning with the ACL guide (Fig. 6). The guide is then moved two to three more times with concurrent drilling as described to achieve appropriate spread within the lesion. Then, the humeral head cartilage should be reinspected to ensure iatrogenic penetration has not occurred.
Outcomes of arthroscopic-assisted technique
Dines et al. [46] reported the outcomes of 3 patients (3 shoulders) that underwent arthroscopic-assisted core decompression as first described by Chapman et al. [53]. Their technique included the use of an ACL tibial drill guide to reduce the risk of articular perforation. All three patients presented with Cruess stage II humeral head AVN based on preoperative radiographs and MRI. At an average follow-up of 9 months (range, 7–11 months), two of three patients had complete resolution of their preoperative pain, and shoulder range of motion was completely restored in three of three patients. One patient presented with persistent pain at the 9-month follow-up, although this was completely resolved with a corticosteroid injection. Long-term outcomes for this technique with and without the use of an ACL tibial drill guide are not currently available for the humeral head.
Adjunctive biologic treatment
More recently, significant focus has been on the concurrent use of growth and differentiation-inducing agents following core decompression to promote native bone regeneration of the decompressed tract. In particular, methods including autologous bone grafting [15], tantalum rod implants [54-56], autologous bone marrow cell implants [57], and synthetic calcium sulfate/calcium phosphate bone cementing [58-64] have been described for core decompression in the femoral head. Although current literature on biologics for core decompression of the humeral head is limited, several techniques have been proposed.
Synthetic bone grafting technique
As presented by Steffensmeier et al. [47], the use of a calcium sulfate and calcium phosphate synthetic bone graft (Pro-Dense, Wright Medical Group, Memphis, TN, USA) is a viable option for adjunctive management with core decompression. Although not sufficiently studied for the humeral head, synthetic bone graft has been proven to promote bone regeneration following femoral head AVN [65,66]. The technique is performed following a standard percutaneous core decompression. Through the original percutaneous incision, an extension cannula is placed at the decompression tract and synthetic bone graft is injected into the proximal humerus (Fig. 7). Fluoroscopy is utilized to visualize complete cementation of the decompression tract. Arthroscopy with irrigation is recommended to ensure no cement is present within the subacromial space.
Outcomes of synthetic bone grafting technique
Steffensmeier et al. [47] reported on one patient (two shoulders) with early-stage AVN of the humeral head who underwent core decompression with synthetic bone graft cement (Pro-Dense, Wright Medical Group). Improvement in pain and range of motion was observed at the final follow-up of 8 months for 1 shoulder and mild residual stiffness was observed at the 4-month follow-up. Neither shoulder progressed to collapse and pain in both shoulders was resolved.
Autologous concentrated bone marrow cell technique
The use of autologous mesenchymal cell grafts for core decompression of the femoral head has been well described. In a meta-analysis by Li et al. [57], improved outcomes were observed in patients receiving congruent mesenchymal injections compared with core decompression alone. Makihara et al. [48] recently showed this technique was a viable adjunctive treatment for core decompression of the humeral head. Bone marrow aspiration, centrifugation, and transplantation were performed according to the technique by Yoshioka et al. [67] for the femoral head. In brief, under general anesthesia, bone marrow aspirate is harvested using a bone marrow biopsy needle with an acid citrate dextrose containing syringe. Centrifugation is performed twice. The first centrifugation is performed at 1,200 ×g for 10 minutes to remove the red blood cell layer. Following a second centrifugation at 3,870 ×g for 7 minutes, the blood plasma is removed, leaving buffy coats containing the mesenchymal cell grafts. After standard percutaneous core decompression, the autologous concentrated bone marrow graft is grafted with a cylindrical rod smaller in diameter than the diameter of the drill to ease implantation. The graft is then implanted within the decompression tract. The procedure is completed by closing the incision using standard technique.
Outcomes of autologous concentrated bone marrow cells technique
Makihara et al. [48] reported four patients (five shoulders) who underwent core decompression for four shoulders with Cruess stage III and 1 shoulder with stage IV AVN of the humeral head using autologous concentrated bone marrow grafts. At an average final follow-up of 49.4 months (range, 24–73 months), the average visual analog scale changed from 33 mm preoperatively to 5 mm postoperatively, and progression to further collapse or TSA did not occur. However, the patient with stage IV shoulder failed to improve following core decompression, requiring TSA prior to the final follow-up. Similarly, Hernigou et al. [68] reported the outcomes of 30 patients (30 shoulders) with adjunctive mesenchymal stem cell injection and 34 patients (34 shoulders) with no adjunctive injection who underwent core decompression for AVN of the humeral head. In the mesenchymal group, 18 patients were pre-collapse and 12 patients were post-collapse. At an average of 7-year follow-up (range, 5–10 years), 3 of 30 patients in the mesenchymal group progressed to humeral head collapse compared with 25 of 34 patients in the untreated group (P<0.0001). In addition, only 2 of 30 patients in the mesenchymal group progressed to shoulder arthroplasty compared with 25 of 34 in the untreated group (P<0.0001).
Bone allograft technique
Galloway et al. [49] described bone allograft in conjunction with core decompression of the humeral head with use of a fibular allograft strut. Bone allograft is used to support the subchondral bone and decrease the risk of articular collapse following AVN lesion decompression rather than bony revascularization [49]. Following a standard arthroscopic-assisted percutaneous core decompression, a bone allograft is prepared with the same diameter of the drilled decompression tract. Introduction of the bone allograft is conducted over the previously placed guide pin and the pin is removed once the graft is secured. The remaining graft is then cut flush with the outer cortex with all edges smoothed using a burr. Galloway et al. [51] recommend under-contouring the graft progressing from proximal to distal to aid with interference fit of the graft within the tract.
Outcomes of bone allograft technique
In a study including 14 pre-collapse shoulders (stage II) and 6 post-collapse shoulders (2 stage III and 4 stage IV), Galloway et al. [49] reported good outcomes for core decompression with adjunctive fibular strut allograft. Prior to the final follow-up, 3 shoulders, including 2 stage II and 1 stage IV, underwent shoulder arthroplasty due to pain. In the pre-collapse group, Shoulder Disability and Shoulder Pain and Disability Index (SPADI) scores were excellent in two shoulders, good in four shoulders, and poor in one shoulder. In contrast, SPADI scores in the post-collapse group included three excellent and one poor result. Limited improvement was observed in range of motion for both groups postoperatively. The better outcome scores in the post-collapse group were attributed to the younger patient age compared with pre-collapse group.
Postoperative protocol
In the literature searched, formal consensus on postoperative restrictions following core decompression was not found. In a few articles, a short period of several days of sling immobilization with early progressive range of motion and limited heavy lifting for 8–12 weeks was recommended [11-13]. Conversely, Steffensmeier et al. [47] recommended no formal postoperative restrictions aside from tolerated activity and Makihara et al. [48] only recommended limiting carrying loads following core decompression. Although postoperative protocols differ, formal evidence indicating the gold standard for postoperative rehabilitation does not exist. However, the concern for postoperative stiffness and functional limitations should be considered with any postoperative protocol. Thus, the authors recommend patients begin a postoperative protocol with early range of motion, including shoulder pendulums, elbow, wrist, and hand exercises, to reduce stiffness. However, restrictions should be guided based on concomitant procedures. If the operation is an isolated core decompression, the authors recommend no formal restrictions and patients allowed to return to their normal activity level as tolerated.
CONCLUSIONS
Core decompression of the humeral head is an excellent treatment modality for shoulder preservation in patients with early-stage AVN of the humeral head without articular collapse. Several techniques have been developed, with good to excellent outcomes for each modality. In theory, a percutaneous, arthroscopic-assisted technique may allow accurate staging and concomitant treatment of intraarticular pathology during surgery, although further long-term clinical studies are necessary to assess the overall outcomes compared with standard techniques. In addition, although use of adjunctive biologics has been well described for core decompression of the hip, further high-quality studies are required in which their benefit in core decompression of the humeral head is further assessed.