INTRODUCTION
Reverse shoulder arthroplasty (RSA) was first introduced as a management option for cuff tear arthropathy (CTA). Its indication has since expanded to include complex proximal humeral fractures (PHFs), and the proportion of such injuries managed with an RSA has increased by nearly threefold in the past decade [1]. Likewise, evidence of good short-term [2,3] and long-term outcomes supports the use of RSA for PHFs [4-6].
This paper compares the outcomes of RSA by diagnosis (traumatic versus atraumatic) in an Asian population. As outcomes, we evaluated the 1-year American Shoulder and Elbow Surgeons (ASES) score, postoperative shoulder ranges of motion, intra- and postoperative complications, 1-year Constant shoulder score, and cumulative revision rate. Our hypothesis was that patients who received RSA for a preoperative diagnosis of trauma would not fare worse than those who received RSA to treat CTA or glenohumeral arthritis (GHOA).
METHODS
This study was approved by Khoo Teck Puat Hospital, Singapore Bioethics Committee (DSRB number 2020/00656). Informed consent was waived. Patients who underwent RSA at our local tertiary institution between January 2013 and December 2019 were included in our study. The main inclusion criterion was primary RSA to treat arthritis or shoulder trauma. The inclusion criteria for the arthritis group were patients who were older than 60 years and suffering from persistently symptomatic and functionally limiting arthropathy of any grade (rotator cuff arthropathy Hamada grade 1ŌĆō5 or glenohumeral arthropathy Walch type AŌĆōD) who had failed on conservative treatment. In the fracture group, the inclusion criteria were patients who were older than 60 years and had a comminuted 3- or 4-part PHF not amenable to fixation; PHFs with head-split; or a PHF-dislocation with a massive rotator cuff tear and significant humeral head bone loss. Other inclusion criteria were primary RSA surgery for any cause and patients with follow-up data for at least 1 year. All procedures were performed by one of four fellowship-trained surgeons (JT, TT, AW, and DT) in the orthopedic surgery department.
Surgical Technique
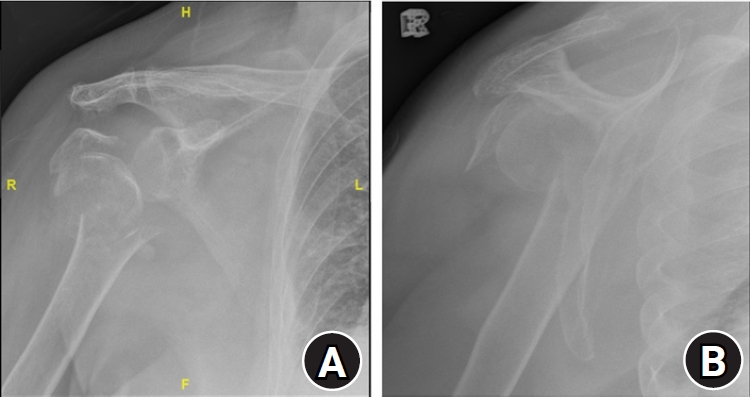
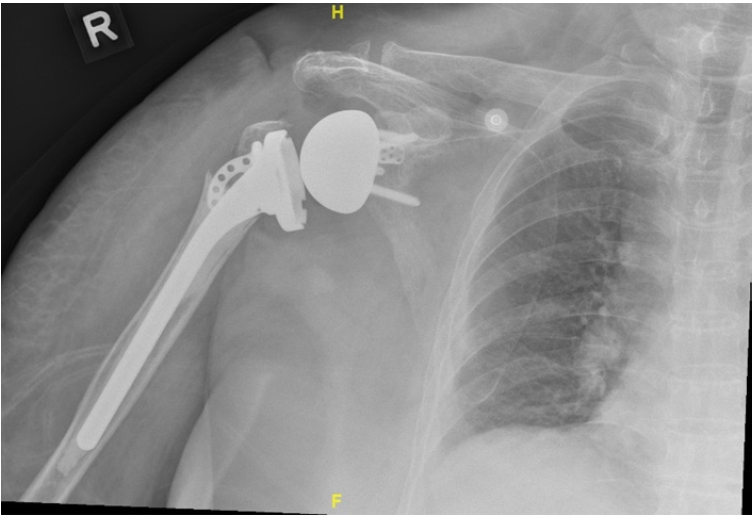
All patients underwent surgery in the beach chair position using a standard deltopectoral approach. The standard procedures for RSA were followed: glenohumeral dislocation, neck cut, glenoid preparation and baseplate insertion, humeral shaft reaming and stem insertion; and finally, tenodesis and tuberosity re-attachment. For CTAs in which the subscapularis tendon was intact, it was peeled from the lesser tuberosity and repaired using the transosseous technique with drill holes into the humerus in 30┬░ external rotation. This step was aborted when the subscapularis was too short to be re-attached to the humerus. For PHFs, efforts were made to preserve the greater and lesser tuberosity fragments, along with the attached rotator cuff tendons (Figs. 1-3). The tuberosities with their attached tendons were similarly repaired using the transosseous technique with 30┬░ external rotation.
Postoperative Rehabilitation Protocol
No external rotation beyond neutral was allowed for 6 weeks if the subscapularis was repaired. Passive range of motion (ROM) exercises were initiated within the first week after surgery under the supervision of a trained physiotherapist. Shoulder strengthening exercises, including active scapular movements and isometric internal and external motion, were allowed as tolerated by pain. Active assisted exercises were gradually initiated beyond the 6th postoperative week. Isometric exercises could slowly include the deltoids. At the 8th postoperative week, graded resistance band exercises for periscapular and shoulder muscles (including shoulder extension, internal rotation, and external rotation) and dynamic stabilization exercises were introduced. Beyond the 12th postoperative week, gradual resistance pressing and pulling movements were introduced with the aim of being functionally independent at light household and work activities.
Data Analysis
The following data were gathered retrospectively from the patientsŌĆÖ electronic medical records: age, sex, indication for RSA, preoperative shoulder ROM, implant type, cement use, and subscapularis tendon repair. Serial postoperative radiographs for up to 1-year, which were performed during follow up visits, were reviewed to assess radiological postoperative complications. The following postoperative outcomes were obtained at the last clinical visit: postoperative ROM, pain scores using a visual analog scale (VAS), the Constant shoulder score, and the ASES shoulder score. The patients were grouped based on preoperative diagnosis. The postoperative outcomes after RSA were compared across the two broad etiologies of trauma and shoulder arthritis.
Descriptive analyses were used to summarize the demographic and clinical characteristics of the patients. For categorical data, frequencies and percentages are presented. For continuous data, the median and interquartile range of the data distributions are presented due to the small sample size and a negatively skewed distribution in the outcome measures. The Shapiro WilkŌĆÖs coefficient (W) was computed to assess whether the data were normally distributed. Data were declared to have a significant skew if the p-value for W was <0.05. Statistical differences in continuous outcomes variables were analyzed using the rank-sum test or Student t-test if the data were non-normally or normally distributed, respectively. For discrete variables, the chi-square test was used to analyze statistical significance unless the number of observations for any category was less than 5; for those categories, PearsonŌĆÖs exact test was used. Statistical significance was declared when a two-sided p-value was <0.05.
RESULTS
A total of 49 patients met the inclusion criteria and was divided into 23 and 26 patients with a preoperative diagnosis of arthritis and trauma, respectively. The groups did not differ significantly by age (72.5 vs. 72.5, p=0.65), sex (female, 52.2% vs. 80.8%, p=0.07), or race (p=0.60). The specific preoperative diagnosis for each group is listed in Table 1. Of the patients who underwent RSA for shoulder arthritis, 82.6% had CTA, and the remaining 17.4% had GHOA. The median follow-up period for the entire cohort was 32.8 months (interquartile range, 12.6ŌĆō66.6), with no significant difference between the groups (31.2 vs. 27.4 months, p=0.64).
The implant used did not differ between the groups (p=0.73) (Table 2), though cemented fracture stems were used for the trauma group, and primary press-fit stems were used for the arthritic group. The use of subscapularis repair (78.3% vs. 88.5%, p=0.45) was also similar in the two groups. A significantly higher percentage of patients undergoing RSA for trauma required cemented fixation compared to those undergoing RSA for arthritis (52.2% vs. 96.2%, p<0.001). The two groups of patients had similar outcomes. The 1-year ASES scores (80 vs. 75, p=0.93) and Constant Shoulder Scores (74 vs. 72, p=0.89) were similar between the groups (Table 4). VAS scores (3 vs. 8, p<0.001) (Table 3) and shoulder ROM scores (abduction angle: 90 vs. 30, p<0.001; forward flexion angle: 90 vs. 30, p = 0.01 at the time of surgery) at the time of surgery were poorer for patients with a preoperative diagnosis of trauma. However, at 12 months, the two groups had similar VAS scores and ROM of the shoulder (p>0.05 for all outcomes).
In terms of complications, the cumulative 7-year revision rate (17.4% vs. 3.8%, p=0.17) did not differ significantly between the two groups. The radiological complications of scapular notching, lucency, and tuberosity migration were similar between the groups (p>0.05 for all outcomes). A significantly higher proportion of patients with a preoperative diagnosis of shoulder arthritis had complications (34.8% vs. 7.7%, p=0.03), and all the dislocations were in the arthritic group (17.4% vs. 0%, p=0.04). A descriptive subgroup analysis was conducted for patients who experienced a complication of any cause. Differences in age; sex; and preoperative ROM in forward flexion, abduction, or external rotation did not account for the higher incidence of complications in the arthritic group (p>0.05 for all variables).
Table 5 highlights the profiles of the four patients who had a postoperative dislocation. The direction of dislocation varied; two of the four patients experienced anterior dislocation postoperatively. All patients had a preoperative diagnosis of CTA. Half of them underwent subscapularis repair during the index surgery, and all used average glenosphere sizes of 36ŌĆō38.
Two of the eight patients (8.7%) who suffered a postoperative complication had partial axillary nerve palsy. One of them had complete spontaneous resolution of symptoms by the third postoperative month. None of the patients in the trauma group experienced an axillary nerve injury.
DISCUSSION
To our knowledge, this is the first retrospective analysis of RSA outcomes from a tertiary institution in Singapore. Regardless of a preoperative diagnosis of arthritis or trauma, the groups had similar demographics at baseline. Patients with a PHF or dislocation had acceptable postoperative results, as did those who suffered from arthritis, in terms of both functional and radiological outcomes. Our results add support to the short-term non-inferiority of using RSA to treat traumatic compared with its traditional indication of CTA.
Previous case series considered the short-term outcomes of RSA to treat trauma. In Cappellari et al.ŌĆÖs study [4] of 91 primary RSAs for PHFs in the elderly, 12 patients reported complications in the first 6 months. Three dislocations occurred and were the only indications for revision surgery in that study. Scapular notching occurred after 6 months in eight patients and was the most notable radiological complication. The short-term outcomes of RSA for trauma are favorable, and intangible advantages that are often unreported include earlier mobilization and reductions in morbidity and in-hospital mortality [4]. However, few studies have directly compared the short-term outcomes of RSA for trauma versus CTA.
The longer-term outcomes of RSA for trauma versus arthritic conditions remain controversial. Coscia et al. [7] reported the largest systematic review of 47 studies on RSAs stratified by preoperative diagnosis. Except for one study, the minimum follow-up period was 24 months. They found that, although RSA provided significant within-group improvements in all outcomes regardless of indication, the acute PHF and PHF sequelae groups consistently showed significantly lower postoperative means of all four standard planes of shoulder motion, as well as lower patient-reported outcome measures (ASES and Constant shoulder), than the groups with GHOA or massive cuff tear with or without GHOA or CTA. Conversely, one of the few long-term prospective studies on RSA for acute fractures versus rotator cuff deficiencies in the elderly, by Sebastia-Forcada et al. [8], showed no significant differences in mean functional scores or ranges of shoulder motion at the end of a mean 8.4 years of follow-up. Only patient satisfaction was significantly lower after RSA performed for PHF (p=0.002). Therefore, it remains debatable whether RSAs used to treat trauma have outcomes comparable to those for arthritic conditions. Moreover, criticizing the use of RSAs to treat trauma would require a holistic comparison of outcomes from the primary fixation of PHFs, and no one has conducted such a study.
The overall complication rate of 20.4% in our cohort is comparable to that in the existing literature [9]. In our series, patients who had a preoperative diagnosis of arthritis had significantly higher rates of complications than those with a preoperative diagnosis of trauma (34.8% vs. 7.7%). Kennedy et al.ŌĆÖs systematic review of 36 studies [10] found that RSAs performed for osteoarthritis of the shoulder had an average pooled incidence of 1.4%, the lowest incidence rate of all pathologies requiring an RSA. However, that finding needs to be interpreted on a background of differing criteria for classification of shoulder pathology that included primary glenohumeral, CTA, and post-traumatic arthritis. Also, the complication rates accumulate as the follow up period becomes longer. Mizuno et al.ŌĆÖs series of 27 RSAs for all-cause GHOA [11], which had an average follow-up duration of 54 months, reported a 15% complication rate. Of the four reported complications in that study, one involved early loosening of the glenoid component, and the remaining three were neurologic complications; no postoperative instability was reported [11]. Existing studies rarely report post-surgical complications stratified by indication. Sebastia-Forcada et al.ŌĆÖs prospective series [8] reported no significant difference in long-term complication rate or 10-year arthroplasty survival between RSA for fracture or for arthropathy. We recognize the higher-than-expected complication rate in the arthritis group in our study. In our series, surgeries were performed by multiple surgeons, so our result could be due to technical error. Overzealous soft-tissue release in arthritic cases can increase the risk of axillary nerve injury and contribute to instability. In one of the cases, part of the anterior acromion was inadvertently excised to facilitate exposure during surgery; in hindsight, that might have precipitated the postoperative dislocation.
Our studyŌĆÖs 7-year prevalence of instability after a primary RSA is 7.55%. All four patients who experienced instability had a preoperative diagnosis of CTA, three of them were males, and half required subscapularis repair. Our prevalence is lower than that reported in Cheung et al.ŌĆÖs multivariate analysis of the independent predictors of post-RSA instability [12]; they reported a 4-year prevalence of 9.24%. They found that being male, having a preoperative diagnosis of fracture, and the absence of subscapularis repair were significant predictors of postoperative instability [12]. All cases of postoperative instability were revised in their series. Gallo et al.ŌĆÖs study of risk factors for post-RSA instability similarly [13] reported a 3-year prevalence of 15.7%. All of their patients had compromised subscapularis tendons at the time of RSA, with seven of the nine patients with instability having had a previous shoulder surgery. The only two patients with instability after a primary RSA both had a preoperative diagnosis of CTA. It is clear that exclusion of revision cases in our study lowered the rates of post-RSA instability reported here. Interestingly, CTA seems to be a risk factor for instability after primary RSA, as supported by our study and Cheung et al. [12], whereas Gallo et al. [13] suggest previous trauma as a risk factor for instability after revision RSA. Although the available literature is divided on whether the preoperative diagnosis is a risk factor for instability, sex, body mass index, and surgical technique are established factors. An aggressive humeral cut, superior glenoid positioning, superior glenosphere inclination, subscapularis repair, and subsequent subscapularis integrity are known surgical missteps that can increase the chance of instability after an RSA [14]. Therefore, attention to surgical details such as soft tissue release and intraoperative assessments of stability are important, regardless of the etiology.
ROM improvements are difficult to compare between arthritic and traumatic indications for RSA given the differences in the underlying conditions. It is clear, however, that RSA can improve the ROM even for chronically arthritic joints. Kim et al. [15] reported a doubling of shoulder forward flexion after RSA for arthritis of any known cause. Likewise, Rhee at al.ŌĆÖs study of primary RSA in CTA [16] found that, after a mean follow-up period of 20.6 months, the mean active forward flexion and external rotation increased significantly, from 96.4┬░ to 138.4┬░ and 30.6┬░ to 48.9┬░, respectively (p<0.001 for both motions). Our outcomes are comparable with those in the existing literature. Some studies have reported worse postoperative ROM and functional outcome scores after RSA for trauma compared with RSA for arthritis [17]. However, the results in our study indicate similar outcomes in the two groups. That might reflect our consistent attempts to reattach the greater and lesser tuberosities when repairing proximal humerus fractures.
Our cohortŌĆÖs combined incidence of notching was 16.3%, less than that reported for the medialized center of rotation (40%ŌĆō90%) [9] but within the wide range (4.6%ŌĆō96%) reported for all RSA regardless of center of rotation [18]. Apart from our choice of lateral offset implants, we pay particular attention to our surgical technique and have a tendency to allow an inferior overhang of the glenoid base plate, which reduces the risk of scapula notching [18]. Our study is, however, limited by the length of the follow-up period. A radiographic analysis by Simovitch et al. [19] showed that the average time required for scapular notching to develop was 51.4┬▒24.1 months, and significantly worse clinical outcomes were found in patients with notching.
Our study is limited by its retrospective nature, and postoperative complications might have been underreported. However, the majority of complications after RSA occur in the early period [20]. Despite a minimum of one year of follow up for all patients included in this study, certain complications, such as glenoid or humeral side loosening, might not have occurred yet. Our results could be further confounded by the possibility that patients included in the trauma group had pre-existing arthritis. However, given the age profile of our patients, it would be challenging to include patients without any signs of arthritis. As the indications for RSA expand, future studies need to be more granular in categorizing the indication for the RSA, such as comparing CTA vs. a massive irreparable cuff tear without arthritis. Patients with a PHF or dislocation did not fare worse than those with arthritis in terms of functional and radiological outcomes 12 months after an RSA. Our complication rate of 20.4% is comparable to that in the literature. Longer-term studies will be useful to confirm the non-inferiority of RSA for trauma compared with the traditional indication of arthritis.