Dynamic three-dimensional shoulder kinematics in patients with massive rotator cuff tears: a comparison of patients with and without subscapularis tears
Article information
Abstract
Background
Massive rotator cuff tears (MRCTs) with subscapularis (SSC) tears cause severe shoulder dysfunction. In the present study, the influence of SSC tears on three-dimensional (3D) shoulder kinematics during scapular plane abduction in patients with MRCTs was examined.
Methods
This study included 15 patients who were divided into two groups: supraspinatus (SSP) and infraspinatus (ISP) tears with SSC tear (torn SSC group: 10 shoulders) or without SSC tear (intact SSC group: 5 shoulders). Single-plane fluoroscopic images during scapular plane elevation and computed tomography (CT)-derived 3D bone models were matched to the fluoroscopic images using two-dimensional (2D)/3D registration techniques. Changes in 3D kinematic results were compared.
Results
The humeral head center at the beginning of arm elevation was significantly higher in the torn SSC group than in the intact SSC group (1.8±3.4 mm vs. −1.1±1.6 mm, p<0.05). In the torn SSC group, the center of the humeral head migrated superiorly, then significantly downward at 60° arm elevation (p<0.05). In the intact SSC group, significant difference was not observed in the superior-inferior translation of the humeral head between the elevation angles.
Conclusions
In cases of MRCTs with a torn SSC, the center of the humeral head showed a superior translation at the initial phase of scapular plane abduction followed by inferior translation. These findings indicate the SSC muscle plays an important role in determining the dynamic stability of the glenohumeral joint in a superior-inferior direction in patients with MRCTs.
INTRODUCTION
Rotator cuff tear is a common shoulder disorder. The main symptoms are pain, restricted range of motion, muscle weakness, and other functional impairments. The primary function of the rotator cuff is to dynamically stabilize the shoulder joint by compressing the humeral head into the glenoid cavity and maintaining the centripetal position of the humeral head [1,2]. Burkhart [3] states that balance of force couples in the transverse and coronal planes is important in maintaining the stability and function of the glenohumeral (GH) joint. The balance of forces in the transverse plane is maintained by the subscapularis (SSC) muscles located anteriorly and the infraspinatus (ISP) and teres minor muscles located posteriorly [1,3]. In the coronal plane, the force couple is mainly formed by the supraspinatus (SSP) and deltoid muscles [4]. Rotator cuff tears disrupt the balance of the force couples, affecting the kinematics of the GH joint, resulting in the loss of ability to elevate the arm [3,5].
Some patients with massive rotator cuff tears (MRCTs) lose the ability to elevate the arm due to secondary changes such as muscle atrophy [6], fatty infiltration [7], and osteoarthritis [8]. This condition is called pseudoparalysis and is associated with abnormal GH joint kinematics, including superior migration of the humeral head on arm elevation [5,9]. Collin et al. [9] classified MRCTs into five types and investigated their relationship to active motion. The authors reported that a tear in the SSP and entire SSC (type B) or SSP, ISP, and superior SSC (type C) were risk factors for developing pseudoparalysis [9]. Furthermore, these patients had difficulty recovering elevation function in a rehabilitation program [10]. Sahara et al. [8] reported that although abnormal GH kinematics were identified in pseudoparalysis, significant difference was not observed in tear type between patients with and without pseudoparalysis. Although SSC tears are considered a risk factor for pseudoparalysis [10], some patients with MRCTs can perform active elevation [8,11]. The influence of SSC tears on GH kinematics in patients with MRCTs without pseudoparalysis is unclear.
In previous studies, cadaveric simulations [4,5], two-dimensional (2D) or three-dimensional (3D) static radiographs [12,13], and dynamic 3D analysis using the 3D-to-2D registration technique were used to measure joint kinematics in rotator cuff tears [8,14-16]. The 3D-to-2D registration technique allows accurate measurement of joint kinematics based on matching a bone model created from computed tomography (CT) images to X-ray fluoroscopic images. High in-plane accuracy is a strong point of these techniques employing single-plane radiographic imaging, with a reported accuracy of 0.47 mm and 1.53 mm for in-plane and out-of-plane translations, respectively, and 0.76° and 3.72° for in-plane and out-of-plane rotations, respectively [17]. In previous studies [14,16] in which this method was used, tear sizes were limited to medium or large rotator cuff tears. To the best of our knowledge, the effects of SSC tears on joint dynamics have not been previously investigated.
Knowledge of the effect of SSC muscle tears on GH kinematics may also provide important information for determining an effective treatment strategy. In the present study, the effects of SSC tears on 3D GH kinematics during scapular plane abduction were examined in patients with MRCTs without pseudoparalysis. We hypothesized that MRCTs with a torn SSC would exhibit greater translation of the humeral head relative to the glenoid cavity than MRCTs without such a tear.
METHODS
This study was conducted in compliance with the principles of the Declaration of Helsinki. The Institutional Review Board of Kyoto Prefectural Rehabilitation Hospital for the Disabled approved the study protocol (No. 11) and all subjects provided their written informed consent before participation.
Subjects
Patients with MRCTs involving at least two tendons, including the SSP and ISP, with or without the SSC, were recruited for the present study. MRCTs were confirmed based on magnetic resonance imaging (MRI) of all patients. Exclusion criteria included a concurrent neuromuscular disorder, a history of shoulder joint surgery, a score >3 on the numerical pain rating scale during arm elevation, and an inability to elevate the arm by at least 140°.
A total of 15 patients (15 shoulders; mean age, 76.1 years) were divided into two groups: 10 shoulders in the SSP and ISP with SSC tears (torn SSC group; mean age, 75.0±7.4 years) and 5 shoulders in the SSP and ISP tears (intact SSC group; mean age, 78.4±2.3 years). The demographic data for the two groups are shown in Table 1.

Demographic, radiographic, and MRI data
Image Evaluation
T1-weighted and T2-weighted MR images were obtained (3.0-T, X-series; Philips Healthcare, Best, the Netherlands). in the coronal oblique, sagittal oblique, and axial planes. The tear sizes were measured using MRI. For the SSP and ISP, the classification by DeOrio and Cofield was used [18]. A massive tear was defined as >5 cm retraction in the coronal plane. For the SSC, the modified Lafosse’s classification [19] was used as follows: type I, a partial tear of the upper one-third of the SSC; type II, a complete tear of the upper one-third of the SSC; type III, a complete tear of the upper two-thirds of the SSC; and type IV, a complete tear of the entire width of the SSC. Fatty infiltration of the SSP, ISP, and SSC muscles was graded using the 5-point semiquantitative scale described originally by Goutallier et al. [7] and modified for MRI analysis by Fuchs et al. [20] as follows: 0, normal; 1, some fat streaks; 2, fatty degeneration <50% but still more muscle than fat; 3, fatty degeneration of 50% (equal fat and muscle); and 4, fatty infiltration >50%. Furthermore, the radiologic evaluation of cuff tear arthropathy was classified into six types according to Hamada et al. [21]: grade 1, acromiohumeral interval (AHI) ≥6 mm; grade 2, AHI ≤5 mm; grade 3, AHI ≤5 mm, with acetabulization; grade 4A, GH arthritis, without acetabulization; grade 4B, GH arthritis, with acetabulization; grade 4A, humeral head collapse, which is characteristic of cuff tear arthropathy. The imaging evaluation data for the two groups are shown in Table 1.
Image Acquisition and 3D Modeling
Scapular plane abduction was recorded using a flat panel radiography/fluoroscopy (R/F) system (Sonialvision Safire, Shimadzu, 0.286×0.286 mm/pixel) and fluoroscopic images were acquired in a single anterior-posterior direction. Patients elevated the arm in the scapular plane (30° anteriorly to the frontal plane) from a natural hanging position to a maximum elevation over 3 seconds, with the elbow joint extended while standing. The distance from the tube of the flat panel R/F system to the target shoulder was 1,500 mm, and the sampling rate was 7.5 frames per second.
CT was then used to obtain 0.5 mm tomographic images of the humerus and scapula. A 3D bone model of the humerus and scapula was created from the tomographic images using segmentation software (3D-Doctor; Able Software Corp., Lexington, MA, USA). The 3D bone models were converted to a polygonal surface model and a smoothing process was applied using a 3D mesh processing software (MeshLab; www.meshlab.net/). A single experienced researcher embedded the local coordinate system of the glenoid and humerus onto the 3D bone models using the 3D-Aligner software (GLAB Corp., Higashihiroshima, Japan). Humerus coordinates were set with their origin at the center of the humeral head, a Y-axis parallel to the humeral shaft, and an X-axis passing through the center of the intertubercular groove [22]. Scapular coordinates were set with their origin at the center of the scapular glenoid cavity, a Y-axis parallel with a line connecting the topmost and lowermost edges of the glenoid cavity, and a Z-axis parallel to a line connecting the anterior-most and posterior-most edges of the glenoid cavity [22].
Model-Image Registration
JointTrack (open-source software; www.sourceforge.net/projected/jointtrack) was used to match the completed 3D bone model with the fluoroscopic images. Outlines in the 3D bone model were matched to outlines in the fluoroscopy images. The greater tubercle, lesser tubercle, humeral head, and humeral shaft were used as landmarks when matching the humerus. The acromial process, coracoid process, glenoid cavity, scapular spine, superior angle, medial margin, and inferior angle were used as landmarks when matching the scapula (Fig. 1).
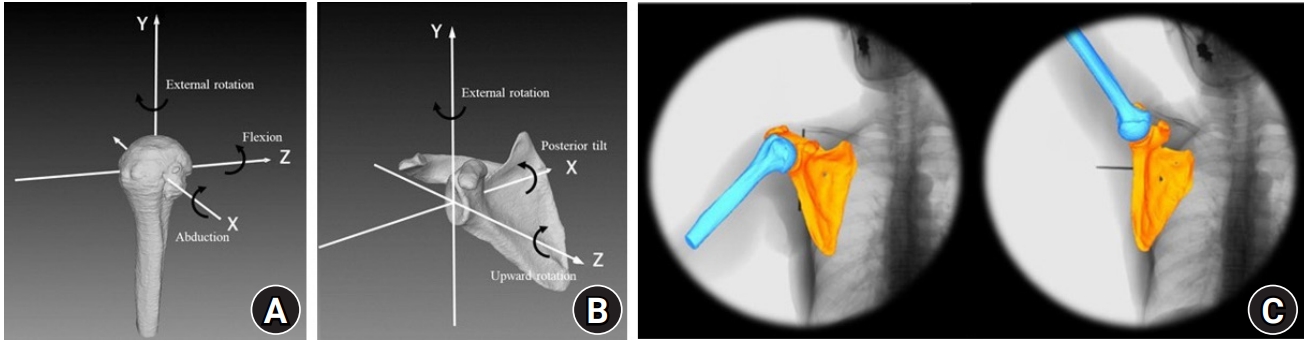
Matching the three-dimensional (3D) bone model and fluoroscopic images. Fluoroscopic images are acquired, a 3D bone model of the humerus (A) and scapula (B) is created using the computed tomography images, and the bone model is matched with outlines on the fluoroscopy images (C).
Data Processing
The 3D shoulder kinematics were obtained using the 3D-Joint Manager software (GLAB Corp.). For the 3D joint orientation, the position of the distal bone in the local coordinate system of the proximal bone was calculated using the Euler angle [23]. Humeral elevation was defined as rotation about the Z-axis. Scapular motion was defined as anterior-posterior tilt about the X-axis, internal-external rotation about the Y-axis, and upward-downward rotation about the Z-axis. Internal-external humeral rotation relative to the scapula was defined as rotation about its Y-axis. The humeral head translation (in the superior-inferior, anterior-posterior, and medial-lateral directions) was calculated as the position of the humeral head center relative to the glenoid center. All kinematics data were measured from the beginning to the end of arm elevation. In addition, translation on each axis was measured three times and the root-mean-square (RMS) error calculated to investigate measurement error. The RMS error observed in this study was an in-plane error of 0.12 mm and an out-of-plane error of 0.61 mm, which are comparable to previous validation studies [17].
Statistical Analysis
Image evaluation and kinematics results were compared between the intact and torn SSC groups. The Mann-Whitney U-test was used to compare age, fatty infiltration, and GH and scapular rotation angles at the beginning and end of arm elevation. Chi-square tests were used to analyze categorical data such as gender and rotator cuff tear arthropathy. The effect of the subject group (torn SSC group and intact SSC group) on the GH kinematics in the three translation directions of the humeral head was analyzed using a two-factor linear mixed-effects model. When a significant interaction between the subject group and arm elevation angle was observed, post hoc Bonferroni correction was used for further significance testing. The software used for statistical processing was IBM SPSS ver. 24 (IBM Corp., Armonk, NY, USA) and the statistical significance level was set at p<0.05.
RESULTS
GH Positions
A significant nonlinear interaction was found for superior-inferior translation between the two independent factors, indicating the subject group effect on superior-inferior translation depended on elevation angle (F=3.85, p<0.05). The humeral head in patients in the torn SSC group was positioned significantly more superiorly than in the intact SSC group at the beginning of arm elevation (−1.1±1.6 mm in the intact SSC group and 1.8±3.4 mm in the torn SSC group, p<0.05). In the torn SSC group, the center of the humeral head had migrated superiorly by 2.3±3.9 mm at 50° arm elevation, then showed significant inferior translation (1.5±3.9 mm) at 60° arm elevation (p<0.05). In the intact SSC group, significant difference was not observed in superior-inferior translation between each arm elevation. Superior-inferior translation of the humeral head during arm elevation is shown in Fig. 2.
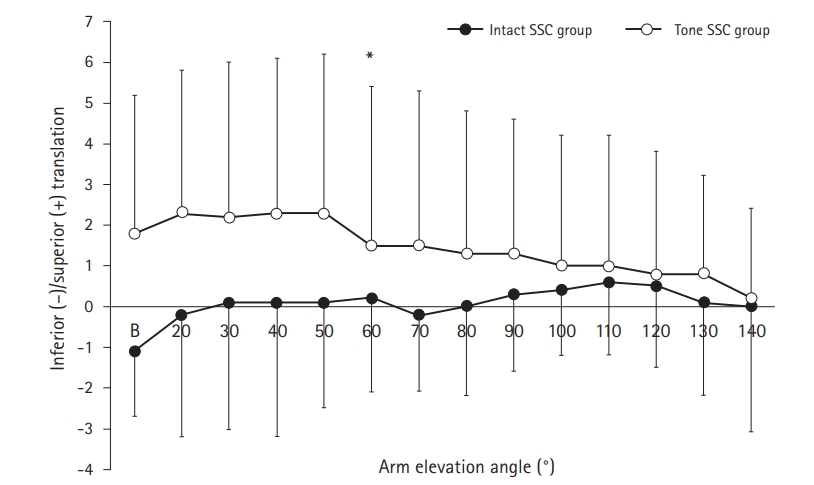
Superior-inferior translation of the humeral head during arm elevation. The mean and standard deviation values are shown for the intact subscapularis (SSC) and tone SSC groups. In the torn SSC group, the center of the humeral head superiorly migrated by 2.3±3.9 mm at 50° arm elevation, which then showed a significant inferior translation (1.5±3.9 mm) at 60° arm elevation (*p<0.05). In the intact SSC group, significant difference was not observed in the superior-inferior translation of the humeral head between the elevation angles. B: beginning of arm elevation.
In both groups, anterior translation relative to the glenoid cavity was observed in the initial phase of arm elevation, then the humeral head gradually migrated posteriorly with increasing elevation (Fig. 3). However, significant interaction was not observed between the two independent factors in the anterior-posterior translation models (F=0.62, p=0.43). Furthermore, significant interaction was not observed between the two independent factors in the medial and lateral translation of the humeral head (F=0.03, p=0.86) (Fig. 4).
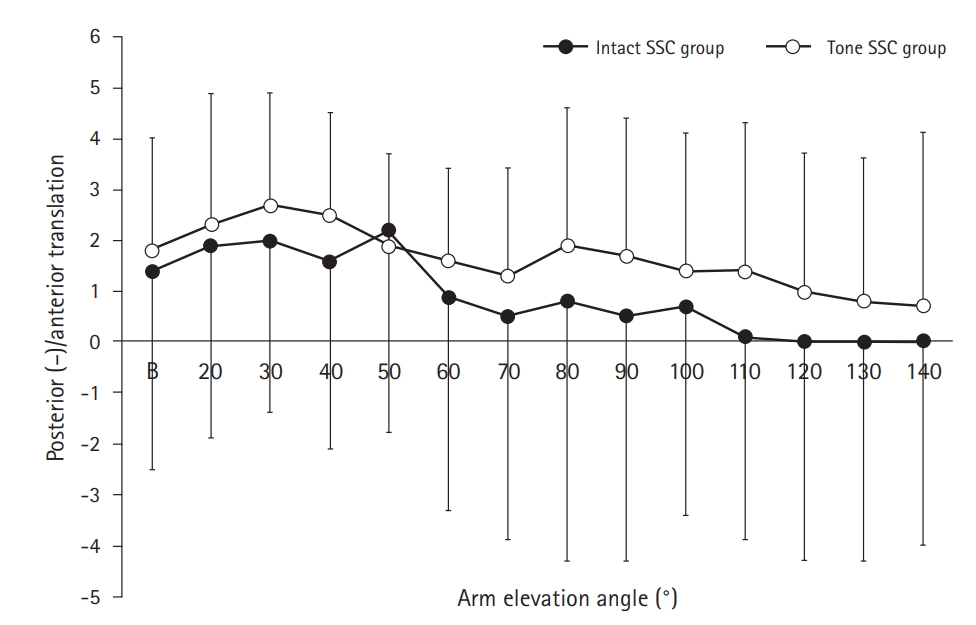
Anterior-posterior translation of the humeral head during arm elevation. The mean and standard deviation values are shown for the intact subscapularis (SSC) and tone SSC groups. Significant difference was not observed between the two groups. B: beginning of arm elevation.
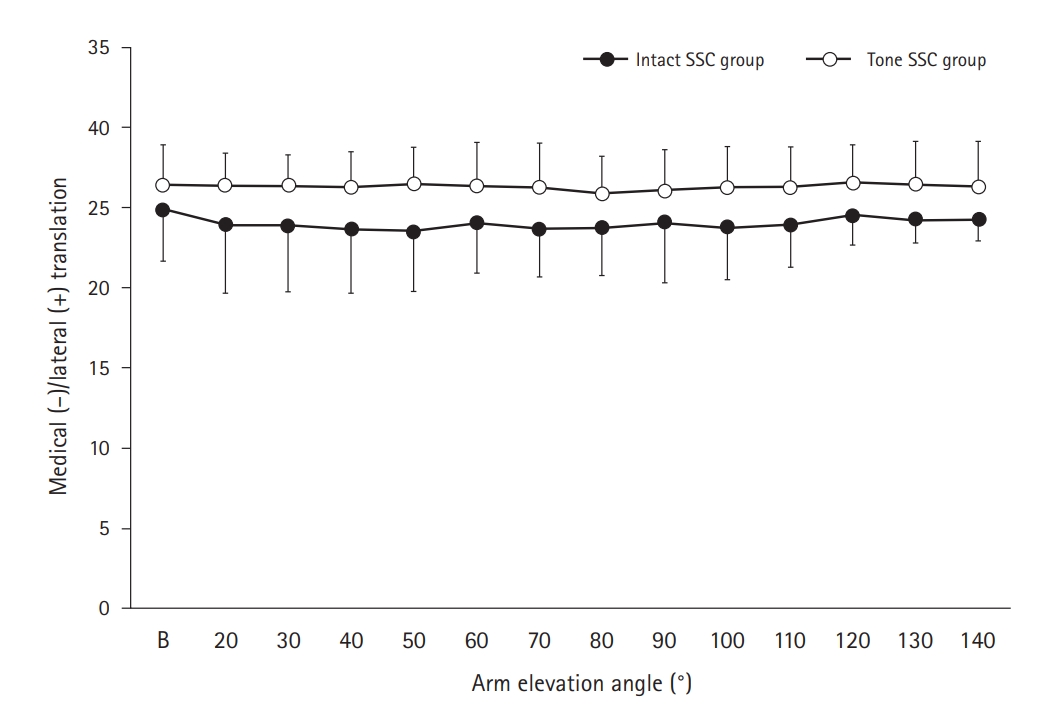
Medial-lateral translation of the humeral head during arm elevation. The mean and standard deviation values are shown for the intact subscapularis (SSC) and tone SSC groups. Significant difference was not observed between the two groups. B: beginning of arm elevation.
Rotation
Significant difference was not found in GH abduction angle between the intact and torn SSC groups at the beginning and end of arm elevation, although the GH abduction angle was slightly smaller in the torn SSC group at the end of elevation (Table 2). Significant difference was not observed between the two groups in the GH external rotation angles at the beginning and end of arm elevation.

Kinematic results
The scapula showed upward rotation, posterior tilting, and external rotation in both groups during arm elevation. The upward scapular rotation at the end of arm elevation was significantly greater in the torn SSC group (52.1°±10.6°) than in the intact SSC group (42.0°±5.5°, p<0.05) (Table 2). However, significant difference was not found at the beginning of elevation. Significant differences in posterior tilting and external scapular rotation were not observed between the two groups at the beginning and end of arm elevation (Table 2).
DISCUSSION
In previous studies, tears of the SSC in MRCTs were reported a risk factor for the development of pseudoparalysis [9,10]. However, in some studies, tear size alone was suggested insufficient to predict the ability to elevate the arm [8,11]. Furthermore, despite the abnormal joint kinematics affecting arm elevation, the effect of SSC tears on GH kinematics remains unclear. In the present study, SSC tear led to greater superior migration of the humeral head center, which then migrated inferiorly as the elevation progressed. To the best of our knowledge, this is the first study in which the effects of SSC tears on GH kinematics were investigated in patients with MRCTs using 3D kinematics analysis with 3D-to-2D registration technique.
Burkhart [3] reported that MRCTs with a torn SSC failed to maintain the coronal plane force couple and showed obvious superior migration of the humeral head into contact with the subacromial surface. These patients showed “captured fulcrum kinematics” in which the undersurface or anterior end of the acromion was used as a fulcrum to elevate the shoulder [3]. In the present study, the humeral head was located significantly more superiorly at the beginning of arm elevation in the torn SSC group than in the intact SSC group. However, the ability to elevate the arm was maintained. This result may support Burkhart’s theory [3] that a superiorly migrated humerus head creates a fulcrum on the acromion’s undersurface.
Regarding the resultant force applied to the humeral head during arm elevation, the vertical force on the glenoid cavity is greatest at 90° elevation and the shear force acting superiorly on the humeral head is greatest between 30° and 60° elevation [2,24]. Because the force of the deltoid muscle causes the upward shearing force on the humeral head to be greatest in the initial phase of the arm elevation, the rotator cuff must exert its greatest force at 60° of elevation and hold the humeral head in the glenoid cavity [2]. In the present study, the humeral head migrated superiorly up to 50° of elevation and inferiorly at 60° of elevation in the torn SSC group, consistent with the importance of the downward action of the humeral head against the upward shear force at 50° to 60° of elevation to enable active elevation in patients with MRCTs with SSC tears.
In contrast, the intact SSC group showed no superior migration of the humeral head relative to the glenoid on arm elevation. Kijima et al. [14] and Millet et al. [16] observed GH kinematics of medium tears with an intact SSC and reported the humeral head did not show significant superior migration in patients with or without symptoms. Kozono et al. [15] found slight superior migration of the humeral head during active arm elevation in patients with large or massive tears (whether these were with or without SSC tears is unknown) compared with healthy subjects. However, significant difference was not found in humeral head position between the two groups. Thus, the presence or absence of SSC tears in patients with MRCTs may affect the dynamic stability of the GH joint in the superior and inferior directions.
Significant difference was not observed in the anterior-posterior and medial-lateral translation of the humeral head between the intact SSC and the torn SSC groups. In cadaveric studies, the effects of rotator cuff tears on GH motion were investigated and tears involving the upper half of the SSC led to anterosuperior translation [25], whereas SSP and ISP tears led to posterior translation [26]. In contrast, Kozono et al. [15] observed anterior-posterior and medial-lateral migration of the humeral head in vivo and found no significant difference between patients with massive tears and healthy subjects. In their study, both groups showed a slight anterior translation after the beginning of arm elevation [15]. In the present study, the humeral head was located anteriorly at the beginning of arm elevation in both groups and gradually migrated posteriorly as elevation progressed. The alterations in GH motion observed in this study may be characteristic of massive tears in vivo.
The torn SSC group had a slightly smaller GH abduction angle and a greater upward rotation of the scapula (i.e., reduced scapulohumeral rhythm) compared with the intact SSC group. Miura et al. [27] measured 3D scapular kinematics in patients with MRCTs and showed the GH abduction angle was significantly smaller and the upward rotation of the scapula was greater than in elderly people without rotator cuff tears. Simulation studies using cadavers showed that as the size of the rotator cuff tear increases, the force required for the deltoid muscle to elevate the arm also increases [28,29]. Furthermore, in electromyographic studies, significantly increased muscle activity was observed in the upper trapezius and the serratus anterior muscle that rotates the scapula in patients with MRCTs [30]. The results of these previous studies [27-30] support our findings and indicate a compensatory increase in upward rotation of the scapula to compensate for the GH abduction torque compromised by the rotator cuff tear.
The present study had several limitations. First, only MRCT subjects capable of active arm elevation were studied. Patients with pseudoparalysis were excluded because humeral head migration was compared at different arm elevation angles. Second, intact rotator cuff and other shoulder muscle activities that affect GH kinematics were not investigated using electromyography or other methods. Finally, a sufficient sample size to improve the statistical power of the study could not be obtained because the target was very severe MRCTs. Electromyographic and simulation analyses are necessary in future studies to investigate the compensatory functions involved in active arm elevation and comparison of joint dynamics with pseudoparalysis patients.
We hypothesized that MRCTs with a torn SSC would exhibit greater translation of the humeral head relative to the glenoid cavity than MRCTs without this type of tear. In cases of MRCT with a torn SSC, the center of the humeral head showed a superior translation at the initial phase of scapular plane abduction followed by inferior translation. These findings indicate the SSC muscle plays an important role in determining the dynamic stability of the GH joint in a superior-inferior direction in patients with MRCTs.
Notes
Financial support
None.
Conflict of interest
None.
Acknowledgements
The authors would like to thank H. Itou for providing technical assistance with the experiments. We also thank Y. Miura and H. Fukushima for their expertise on shoulder rehabilitation.