Delayed surgical repair of the deltoid following acromioplasty: a case report
Article information
Abstract
Currently, the literature contains few studies that describe any potential complications following arthroscopic acromioplasty. Because part of the anterior deltoid originates from the anterior acromion, there is a risk for violation and subsequent iatrogenic rupture or avulsion during this procedure. This type of injury can be a devastating problem for patients that may lead to poor function and debilitating pain. We present a patient with deltoid insufficiency following arthroscopic acromioplasty who elected to proceed with operative management with a planned arthroscopic evaluation of the shoulder followed by an open deltoid repair. At the final follow-up visit 2.5 years postoperatively, the patient reported improved pain from baseline and no residual disability and was able to perform most activities of daily living without difficulty. This case serves as an example of a surgical repair for a deltoid avulsion following arthroscopic acromioplasty. As there is still a lack of standard guidelines, our suture repair technique can be considered one method of treatment for this type of injury.
The deltoid muscle is divided into anterior, middle, and posterior components. While the loss of strength generated by the posterior deltoid may be compensated by other muscles (such as the latissimus dorsi), the loss of the anterior deltoid can be debilitating for patients as it is responsible for approximately 50% of the strength involved in elevating the arm within the scapular plane [1].
Subacromial impingement or rotator cuff tendinopathy is a common cause of shoulder pain and accounts for 44%–65% of shoulder pathology [2]. Patients often report pronounced pain that is exacerbated by motions commonly utilized for many activities of daily living (ADL). In 1972, Neer [3] first described the open anterior acromioplasty technique for patients with shoulder impingement; this procedure was later extended by Rockwood and Lyons [4], who recommended further resection beyond the anterior edge of the clavicle to account for any residual anterior impingement. Importantly, both studies highlighted the significance of restoring the integrity of the deltoid muscle to the acromion, especially in regards to the anterior component [3,4].
The rates of acromioplasties being performed are increasing yearly. One study reviewed the number of acromioplasties that took place over a 10-year-period from 1996 to 2006 and observed a three-fold increase with only a 75% increase in all other orthopedic procedures [5]. There is limited orthopedic literature that currently describes the potential complications that can arise following acromioplasty. With 25% of the anterior deltoid originating from the anterior acromion, there is a potential risk for violation of the anterior deltoid and subsequent iatrogenic rupture or avulsion [6-8]. This injury can be a devastating problem for patients and may lead to pain and decreased function. We present a patient found to have deltoid insufficiency following acromioplasty who was treated with open surgical repair and clinically followed-up over 2.5 years postoperatively.
CASE REPORT
Initial Evaluation
The patient was a 38-year-old, right-hand-dominant male who reported 1 year of persistent left shoulder pain. He was referred for further management following arthroscopic debridement, biceps tenotomy, and acromioplasty 6 months ago. His prior management included a single cortisone injection. The patient’s initial history revealed progressive shoulder pain rated as an eight out of 10 that “wakes the patient from sleep.” Furthermore, the patient reported pain, loss of strength, and notable weakness with abduction. This patient’s initial American Shoulder and Elbow Surgeons (ASES) shoulder score was 5.
Upon initial physical examination, pertinent positive findings included tenderness to palpation of the left anterior acromion with obvious soft tissue deficiency around the deltoid. The range of motion was notable for active elevation to 130° and active external rotation to 40° on the left, compared to active elevation of 160° and active external rotation to 70° on the right. Anterior deltoid and rotator cuff strength were noted to be 4/5 with painful impingement maneuvers and restricted motion with true abduction. The patient’s strength was 5/5 and was without limitation for the contralateral upper extremity. All other available imaging, including plain radiographs (Fig. 1) and magnetic resonance imaging (Fig. 2), was reviewed and was consistent with a resected acromion, avulsion of parts of the anterior and middle head of the deltoid, and subacromial bursal fluid.
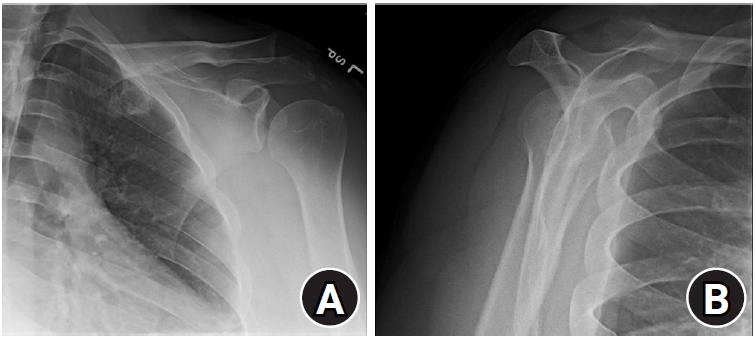
Grashey view (A) and scapular Y view (B) depicting the left shoulder following arthroscopic acromioplasty at the patient’s initial presentation for treatment.

(A-C) Magnetic resonance imaging of different sections depicting avulsed anterior and middle heads of the deltoid muscle following arthroscopic acromioplasty.
Operative Management: Arthroscopic
Treatment options were discussed with the patient, and he elected to proceed with operative management with a planned arthroscopic evaluation of the shoulder followed by open deltoid repair. An interscalene block was utilized for regional analgesia, and the patient was brought into a beach chair position after the induction of general anesthesia. An initial diagnostic evaluation of the glenohumeral joint was completed through a conventional posterior portal (Fig. 3) to rule out any potential rotator cuff pathology and arthrofibrosis intraarticularly that would not be as easily assessable through an open approach. The glenohumeral surfaces were noted to be intact with minimal chondromalacia, some evidence of labral fraying, and a surgically absent biceps tendon. An anterior portal was used to debride the synovium and frayed superior labrum. The articular surfaces of the supraspinatus, infraspinatus, and subscapularis were intact. Next, the subacromial space was evaluated, and significant debris was debrided. There was fraying of the rotator cuff, but no focal areas necessitated repair. A 4.5-cm deltoid defect was identified arthroscopically. An ablation device was used to clear the undersurface of the acromion, allowing for identification of the anterior edge. At this juncture, the arthroscopic debridement was completed, and then attention was turned to the open repair.
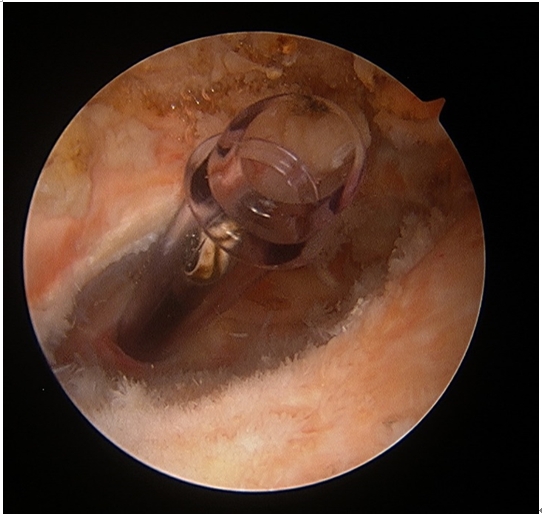
An arthroscopic view of the glenohumeral space upon access via a conventional posterior portal.
Operative Management: Open
An incision was made over the area of the deltoid defect. The skin and subcutaneous tissue were divided to the level of the deltoid fascia. All fibrous tissue that did not appear normal was resected, exposing the deltoid defect at the anterior portion of the previously resected acromion and at the medial portion of the clavicle. The end of the clavicle and the remainder of the acromion were decorticated. Eight drill holes were made through the acromion and clavicle, and #2 Ethibond sutures (Ethicon, Cincinnati, OH, USA) were passed through these holes. The anterior deltoid was mobilized, and the sutures were passed through in a modified Mason-Allen fashion (Fig. 4). The sutures provided good approximation of the deltoid to the bony surfaces (Fig. 5). Fig. 6 shows a step-by-step schematic drawing that is provided for visual representation of this repair technique. We used 0 Vicryl (Ethicon) to further secure the deltoid trapezial fascia. The wound was thoroughly irrigated, and the skin was closed with 2-0 Vicryl and 4-0 Monocryl (Ethicon).

Repair sutures were passed through in a modified Mason-Allen fashion.

An appropriate approximation of the deltoid to the bony surface was achieved.
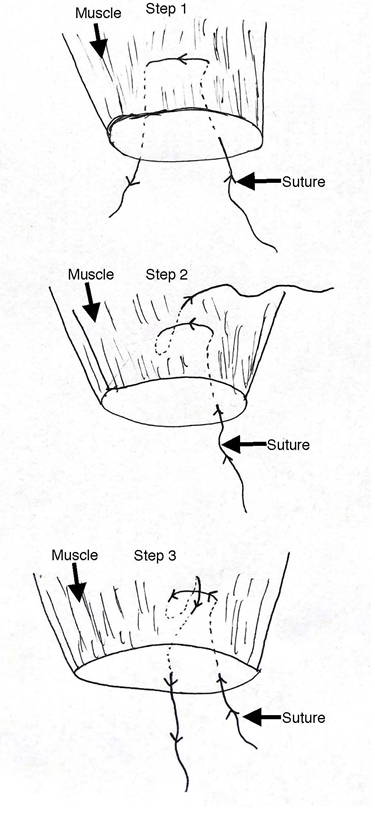
A schematic drawing of the steps involved in an open deltoid repair.
Hospital Course and Follow-up
In the immediate postoperative period, the patient was instructed to avoid all active range of motion activities, maintain the use of an abduction brace, and perform pendulum exercises. Postoperatively, the patient began formal physical therapy at 4 weeks and was granted an unrestricted active range of motion at 6 weeks.
The treating fellowship-trained shoulder and elbow surgeon assessed the patient’s pain level through the visual analog scale as well as his functional and strength status using the ASES shoulder score at routine postoperative clinic visits. In addition, a thorough history and physical exam were conducted at each postoperative follow-up visit. At 3 months postoperatively, the patient’s range of motion was measured to an active elevation and external rotation of 176° (△ +46°) and 75° (△ +35°), respectively. However, the patient’s strength remained unchanged from the initial preoperative assessment. At the final follow-up appointment 2.5 years postoperatively, the patient reported minimal to no pain at baseline and exacerbated 6/10 pain with certain activities, such as sleeping on the affected side. Further, he reported minimal to no restriction in his range of motion and had experienced significant improvement from baseline in his strength and ability to perform necessary ADLs. The final ASES shoulder score was 61 (△ +56).
DISCUSSION
The deltoid muscle plays an important role in motion that occurs near the glenohumeral joint. Although it shares its origins with the clavicle, acromion, and scapular spine, the superior surface of the acromion is the primary origin for the anterolateral or middle head of the deltoid. Deltoid rupture can lead to progressive pain and loss of function in patients’ ADLs. Frequently, patients will fail non-operative management, which can include nonsteroidal anti-inflammatories, narcotic medications, and aggressive physical therapy. In such a case, there is a strong indication for operative intervention [1].
We have presented the case of a patient who reported a restricted range of motion and progressive shoulder pain for the past 1 year. Advanced imaging revealed an avulsed middle head of the deltoid 6 months status post-arthroscopic acromioplasty. Our review of the literature yielded multiple cases that described deltoid repairs following open procedures. For example, Gumina et al. [7] reported deltoid repairs in two patients following open rotator cuff repair, with each occurring within 1 month of the diagnosis of deltoid rupture.
Although several reports in the literature have recognized the risk of deltoid avulsion following open acromioplasty, the data associated with an arthroscopic approach have been limited due to this condition’s infrequent occurrence [4,9]. Bonsell [10] reported one case of deltoid rupture following arthroscopic subacromial decompression. Rupture was hypothesized to have occurred secondary to over-resection of the acromion, which weakened the origin of the deltoid. Another association with rupture of the deltoid was noted by Yamaguchi et al. [8], who cited the frequent use of steroid injections as a contributing factor for spontaneous deltoid rupture. Factors that likely contributed to deltoid rupture in this case included our patient’s previous cortisone injection along with his history of aggressive acromial resection.
The patient in this study was found to have a significant deltoid defect upon arthroscopic evaluation. The size of the defect was postulated to have a direct effect on the level of pain and the functional deficits that were observed at this patient’s initial evaluation. The repair of our patient’s deltoid was uncomplicated and was performed with primary suture anchors to the acromion and clavicle. With an extensive physical therapy protocol, our patient experienced improvement in active elevation and also in active external rotation. After 2.5 years, the patient reported minimal to no pain with most of his ADLs and significant improvement from his baseline pain score (8/10). Despite still reporting periodic pain during sleep, the patient was overtly satisfied with his surgical outcome.
Our study was limited in that the index arthroscopic acromioplasty was done at an outside institution and by a different surgeon than the one who treated the patient’s deltoid insufficiency. Consequently, there was limited access to this patient’s prior surgical information, including the technique used for acromioplasty, the initial treating surgeon’s level of expertise, and any existing concomitant pathologies that may have been located near the anterior acromion.
This case is an example of a successful surgical repair of deltoid avulsion following arthroscopic acromioplasty. Extensive research demonstrates the importance of the deltoid and the necessity for its repair following detachment. The insufficient number of reported cases explain the current lack of standard guidelines for this type of injury. Furthermore, unlike in open acromioplasty, where there can be visual confirmation regarding the integrity of the deltoid, the arthroscopic approach has a higher chance of undetected deltoid insufficiency. In these cases, our suture repair technique should be considered to treat iatrogenic deltoid rupture.
Notes
Financial support
None.
Conflict of interest
None.