Intraoperative periprosthetic humeral fracture during reverse shoulder arthroplasty: a sequelae of prior biceps tenodesis
Article information

Abstract
Intraoperative periprosthetic humeral fractures are a rare but debilitating complication of reverse shoulder arthroplasty and can occur during multiple stages of the procedure. Prior biceps tenodesis has been found to reduce cortical humeral strength and predispose the patient to humeral fracture. We present a case of a 68-year-old female with a previous history of biceps tenodesis due to an irreparable rotator cuff tear. Months later, and after symptoms persisted, a reverse shoulder arthroplasty was performed. During the surgery and while performing final reduction, a fracture line was observed involving the hole used for the previous tenodesis procedure. The fracture was repaired, and the patient reported favorable outcomes. We report several factors that might have contributed to sustenance of this intraoperative fracture including prior biceps tenodesis, use of a press fit humeral stem, and the sex of the patient.
Level of evidence: V.
Intraoperative periprosthetic humeral fractures have been reported to occur in 1.5% of shoulder arthroplasties [1]. They can occur during humeral preparation, implant insertion, or shoulder reduction. Reverse shoulder arthroplasty, introduced in 1987, gained popularity for treatment of cuff tear arthropathy, proximal humerus fracture and revision shoulder arthroplasty [2]. With these rising trends, multiples studies have assessed the rate and risk factors of fractures associated with reverse shoulder arthroplasty. To our knowledge however, there have been no reports of intraoperative humeral fractures during reverse shoulder arthroplasty, associated with prior biceps tenodesis.
CASE REPORT
The patient was a 68-year-old female who underwent shoulder arthroscopy and biceps tenodesis for a painful irreparable rotator cuff on January 29, 2019. The Patient provided consent for her case to be reported in this study; as such all relevant data were deidentified, anonymized and included in this case presentation. Tenodesis was performed in a subpectoral position using an all-suture anchor with a 1.8-mm-pilot drill hole to minimize bone loss. The patient failed to improve significantly, and we proceeded with a reverse prosthesis on March 10, 2020. X-ray imaging performed prior to the reverse shoulder arthroplasty clearly revealed the tenodesis hole of the prior procedure (Fig. 1).

X-ray showing the biceps tenodesis hole (arrow) prior to reverse shoulder arthroplasty in the patient.
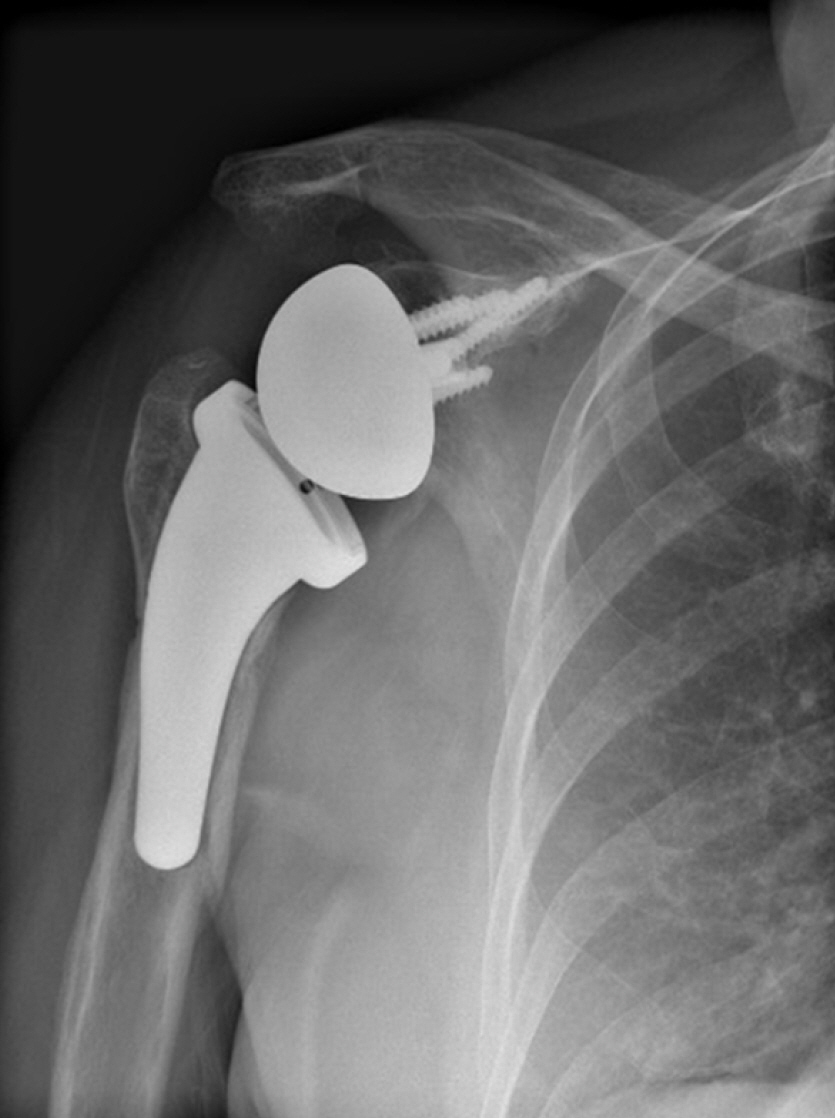
Arthroplasty was performed through a deltopectoral approach using the Aequalis Ascend Flex reverse shoulder system from Wright Medical (Memphis, TN, USA). The surgery was uneventful, and the final reduction was performed using a 6-mm insert for the humeral tray (smallest option). After reduction was achieved, the humeral stem was unstable, and an oblique fracture line was identified involving the site of the osteotomy and exiting through the hole used for anchoring the biceps. An intraoperative X-ray of the shoulder is shown in Fig. 2. The stem was removed, and the fracture was fixed by cerclage using two non-absorbable sutures. The stem was inserted and found to be stable before and after reduction with a 6-mm liner. The procedure was uncomplicated, and the patient wore an arm sling for 2 weeks. Follow-up at 5 months from surgery revealed a stable implant with a good location and good bone healing (Fig. 3).

Intraoperative X-ray showing an oblique fracture of the humerus (arrow) in the patient.
X-ray of the shoulder at 5-month follow-up showing a stable implant in a good location with good bone healing.
DISCUSSION
Pathologies targeting the long head of the biceps (LHB) are observed frequently and concomitantly with rotator cuff tear [3]. Indications for tenodesis have been inconsistent in the literature. Nevertheless, the procedure can be recommended when there is partial tearing, instability, or tenosynovitis of the LHB tendon [4]. Other conditions include SLAP tear and LHB pain upon physical examination [4]. In the setting of irreparable rotator cuff tears, a study by Walch et al. [5] explored the outcomes of 307 arthroscopic biceps tenotomies following irreparable full-thickness tears and reported favorable results with a low rate of complications. Moreover, the American Academy of Orthopedic Surgery recommends biceps tenodesis or tenotomy with low strength for patients with irreparable rotator cuff tear similar to our patient [6].
Tenodesis techniques involve the usage of metal anchors or bone tunnels, and this can create areas of potential weaknesses that predispose the proximal humerus to fracture under stress. Previous cases have described such a complication post biceps tenodesis, and these have been presented in Table 1 [7-13]. It had been suggested in cadaveric literature that interference screws in biceps tenodesis procedures provide better fixation compared to all-suture anchors. However, more recent studies concluded that both techniques are reliable for both supra-pectoral and subpectoral tenodesis [14,15]. Nevertheless, the rate of fracture-related complications is higher with interference screws, which employ bi-cortical drilling, compared to all suture anchors where smaller bore-drill holes are used to minimize bone loss [14,15]. Given that our case involved an elderly woman with a high risk of osteoporosis, we opted to perform tenodesis using an all-suture anchor.
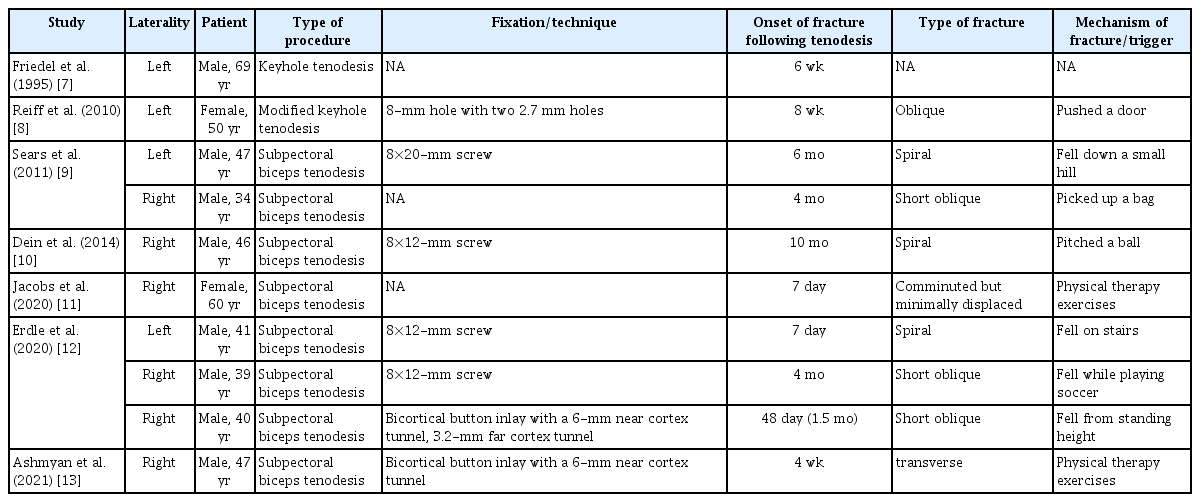
Cases of humeral fractures post biceps tenodesis reported in the literature
Humeral fractures following tenodesis can occur days to months following the procedure due to trivial trauma or triggers (Table 1) [7-13]. The size of the hole relative to bone diameter has been found to have an antagonistic effect on bone strength [16]. Studies on femur models have shown that drill holes can decrease torsional bone strength by up to 40% for small holes and as much as 62% in larger holes (one-fifth of the bone diameter) [16]. In tenodesis procedures that utilize interference screws, even a 6.5-mm drilling hole could reduce the torsional strength of the humerus by 30% compared to that of the controls [17]. In our case, the patient had previously undergone a biceps tenodesis using an all-suture anchor; even though this technique minimizes bone loss compared to interference screws, the intervention can produce compromised bone integrity and increased risk of fracture during insertion of the reverse shoulder arthroplasty prosthesis. Another highly possible contributing factor was the use of a press fit humeral stem. As demonstrated in a cadaveric study by Lee et al. [18], sequential cylindrical reaming required to achieve substantial cortical contact preferentially removes the anterior and posterior cortices. This creates weak areas prone to fracture during stem impaction or shoulder reduction intraoperative. The association between press fit implants and intraoperative humeral fractures was demonstrated in a study by Athwal et al. [1]. This was supported by the higher rate of postoperative periprosthetic fractures in patients with uncemented stem fixation reported by King et al. [19] even though statistical significance was not achieved. In our case, the proximal humeral fracture occurred during reduction, which further suggests that the biomechanics of injury were due to an unbalanced force transmission during press fitting and stem impact rather than torsional stress reduction as seen in other reported cases in the literature, where more bone-compromising techniques were used during biceps tenodesis (Table 1).
Other factors might have contributed to this complication. The patient’s female sex could have predisposed her to fracture. One study published by Wagner et al. [20] explored multiple risk factors for fracture occurrence in revision reverse total shoulder arthroplasty. Female sex was considered to be a significant risk factor to fracture occurrence, probably due to the higher rate of osteoporosis in the female population, where osteoporosis is four times more prevalent compared to men [20,21]. While other cases reported in the literature involved only males, our patient was an elderly female, and her risk of osteoporosis was prominently high [21].
The periprosthetic fracture was fixed intraoperatively in our patient using a suture cerclage. Several studies have asserted and emphasized the efficiency and safety of using a suture cerclage rather than a stainless steel wire or other methods of fixation [22-24]. This was supported further by the uneventful postoperative course of our patient, who exhibited good bone healing and stability on follow-up (Fig. 3).
Few case reports presenting this postoperative complication exist in the literature. While our case presents that of only one patient, to our knowledge, it is the first to present a fracture after an all-suture anchor biceps tenodesis and during a reverse shoulder arthroplasty. Additional research and studies regarding the biomechanics of biceps tenodesis techniques are needed to better understand the sequelae of this procedure on humeral bone integrity and to help prevent such complications in the future.
DISCUSSION
In conclusion, further studies are required to better evaluate the role of prior biceps tenodesis in fracture development and establish potential causality. Our report helps shed light on certain factors that influence postoperative course and reduce the rate of complications following biceps tenodesis. Biceps tenodesis techniques should be suited to individual cases to help preserve bone integrity in patients with high risk of osteoporosis. In addition, when operating on a patient with previous biceps tenodesis, additional care should be taken to help prevent perioperative fractures such as that reported in our case. Sex, prior biceps tenodesis, and fracture risk should be addressed when employing maneuvers that compromise bone integrity and apply stress on the proximal humerus. This highlights another area of interest of evaluation of methods of fixation and their effects on fracture development.
Notes
Author contributions
Data curation: SS, HB. Investigation: SS, HB. Methodology: HB. Project administration: HB. Supervision: HB. Visualization: HB. Writing – original draft: SS, MYF. Writing – review & editing: SS, MYF, HB.
Conflict of interest
None.
Funding
None.
Data availability
None.
Acknowledgments
None.