Determining the incidence and risk factors for short-term complications following distal biceps tendon repair
Article information

Abstract
Background
Distal biceps rupture is a relatively uncommon injury that can significantly affect quality of life. Early complications following biceps tendon repair are not well described in the literature. This study utilizes a national surgical database to determine the incidence of and predictors for short-term complications following distal biceps tendon repair.
Methods
The American College of Surgeons’ National Surgical Quality Improvement Program database was used to identify patients undergoing distal biceps repair between January 1, 2011, and December 31, 2017. Patient demographic variables of sex, age, body mass index, American Society of Anesthesiologists class, functional status, and several comorbidities were collected for each patient, along with 30-day postoperative complications. Binary logistic regression was used to calculate risk ratios for these complications using patient predictor variables.
Results
Early postoperative surgical complications (0.5%)—which were mostly infections (0.4%)—and medical complications (0.3%) were rare. A readmission risk factor was diabetes (risk ratio [RR], 4.238; 95% confidence interval [CI], 1.180–15.218). Non-home discharge risk factors were smoking (RR, 3.006; 95% CI, 1.123–8.044) and ≥60 years of age (RR, 4.150; 95% CI, 1.611– 10.686). Maleness was protective for medical complications (RR, 0.024; 95% CI, 0.005–0.126). Surgical complication risk factors were obese class II (RR, 4.120; 95% CI, 1.123–15.120), chronic obstructive pulmonary disease (COPD; RR, 21.981; 95% CI, 3.719–129.924), and inpatient surgery (RR, 8.606; 95% CI, 2.266–32.689).
Conclusions
Complication rates after distal biceps repair are low. Various patient demographics, medical comorbidities, and surgical factors were all predictive of short-term complications.
INTRODUCTION
Distal biceps tendon rupture represents three percent of all biceps tendon injuries and occurs at an incidence of 1.2–5.4/100,000/yr [1-3]. Injury typically occurs under mechanical stress during eccentric muscle contraction in middle-aged males and athletes [2,3]. Although relatively uncommon, distal biceps tendon rupture can significantly impact quality of life. Nonoperative treatment can result in loss of elbow flexion and endurance, as well as a 40% decrease in supination strength [1,4,5]. Several surgical approaches have been described, including a single- or double-incision technique, and various fixation methods can be considered for operative repair of the biceps tendon to the radial tuberosity [1,6].
Regardless of the surgical approach or fixation method selected, excellent clinical outcomes are reported. A study of distal biceps rupture within the military population found that 96.6% of patients who underwent operation returned to unrestricted preoperative military functions [7]. However, operative treatment is associated with potential risks, such as re-rupture or significant postoperative elbow dysfunction, which should be discussed with patients when obtaining informed consent.
A recent systematic review of complications after distal biceps tendon repair reports a 25% overall and 4.6% major complication rate. The most common major complications in order of prevalence are posterior interosseous nerve injury, median nerve injury, re-rupture, and synostosis [8]. Several studies have investigated factors that increase the risk of distal biceps rupture. Tobacco use was found to result in a 7.5-fold increase of distal biceps tendon rupture risk [3]. Other previously identified risk factors for distal biceps rupture include elevated body mass index (BMI), anabolic androgenic steroid use, and pre-existing tendinosis or mucoid degeneration [2,9,10].
Although these findings are helpful for identifying patients at risk of rupture, there is a lack of literature that identifies factors related to short-term complications and quality of care—including unplanned readmission, reoperation, non-home discharge, and prolonged hospital length of stay. This study aims to utilize a verified national surgical database to determine the incidence of and predictors for various short-term complications following distal biceps tendon repair. We hypothesize these risk factors to include older age, elevated BMI, and various comorbidities such as diabetes and smoking.
METHODS
The applicable institutional review board deemed an IRB exemption for our analysis of the NSQIP database due to the retrospective nature and prior de-identification of the NSQIP registry.
Data Source
All data discussed herein were obtained from the American College of Surgeons’ National Surgical Quality Improvement Program (ACS NSQIP) database. The ACS NSQIP is a validated and Health Insurance Portability and Accountability Act-compliant database that provides deidentified surgical outcomes data from several hundred participating hospitals in the United States, annually. In the year 2017, there were 708 participating institutions that provided data for over one million surgical cases in total. The ACS NSQIP have implemented regular auditing procedures that have yielded data with excellent reliability that has continued to improve over time [11]. Additionally, the database has been utilized extensively to identify the incidence of and risk factors for a variety of short-term complications following a variety of orthopaedic procedures [12-14].
Search and Inclusion Criteria
The ACS NSQIP database was used to identify patients undergoing distal biceps repair between January 1, 2011, and December 31, 2017, using Current Procedural Terminology (CPT) code 24342. Cases with concurrent procedures, as determined by concurrent reported CPT codes, were excluded from the final analysis. Any case with incomplete data was also excluded from the final analysis.
Risk Factors
Patient demographic variables of sex, age, BMI, American Society of Anesthesiologists (ASA) class, functional status, and several comorbidities were reported for each patient. The following comorbidities were included in the analysis—diabetes, smoking, chronic obstructive pulmonary disease (COPD), congestive heart failure, hypertension, dialysis use, chronic steroid use, and bleeding disorders.
Complication Measures
The incidence of several 30-day complications, including unplanned readmission, reoperation secondary to distal biceps tendon re-rupture, non-home discharge, mortality, and several medical and surgical complications were assessed in this population. The medical complications analyzed were pneumonia, pulmonary embolism, urinary tract infection, cardiac arrest, and systemic sepsis. Surgical complications included incision dehiscence and surgical site infections. Functional status was defined using three categories: independent in activities of daily living (ADL), partially independent, and dependent requiring assistance with ADL. All complications were reported within the first 30 days postoperatively.
Statistical Analysis
The incidence of 30-day complications was reported as a percentage of the entire cohort. Multivariate logistic regression was used to identify independent risk factors associated with the various complications of interest (e.g., unplanned readmission, reoperation secondary to distal biceps tendon re-rupture, mortality, non-home discharge, medical complications, and surgical complications). Statistical significance was pre-determined to be p<0.05. All statistical tests were completed using IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The final cohort comprised 2,169 patients. The largest number of patients was male (97.7%), age 40-50 years (36.7%), BMI overweight class (37.2%), ASA class 2 (56.1%), and functionally independent (99.5%). The most prevalent comorbidities were hypertension (25%), smoking (14.8%), and diabetes (5.7%) (Table 1). The majority of patients underwent general anesthesia (91.5%), had an operative time of 60–120 minutes (58.0%), and were outpatients (93.8%) (Table 2).
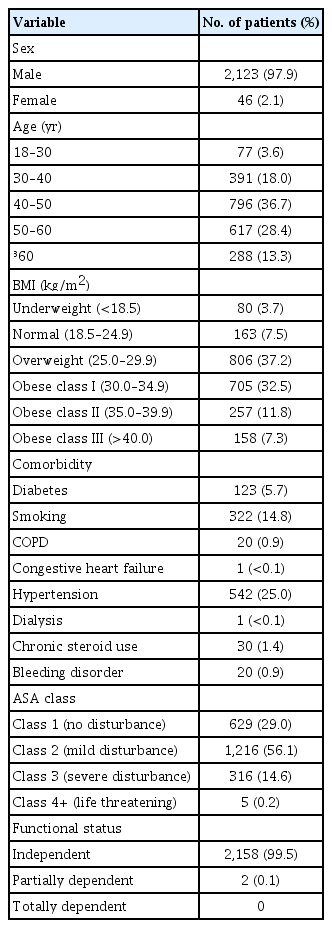
Demographics and comorbidities of included patients

Surgical and hospital course of included patients
Overall 30-day complications included readmission (0.7%), reoperation secondary to distal biceps tendon re-rupture (0.6%), non-home discharge (1.0%), mortality (<0.1%), surgical complications (0.5%), and medical complications (0.3%). The most common surgical and medical complications were superficial surgical site infections (0.2%) and urinary tract infections (0.2%), respectively (Table 3). A risk factor for readmission was diabetes (risk ratio [RR], 4.238; 95% confidence interval [CI], 1.180–15.218). Risk factors for non-home discharge were smoking (RR, 3.006; 95% CI, 1.123 – 8.044]) and age ≥60 years (RR, 4.150; 95% CI, 1.611–10.686). Being male was protective for medical complications (RR, 0.024; 95% CI, 0.005–0.126). Risk factors for surgical complications were obese class II (RR, 4.120; 95% CI, 1.123–15.120), COPD (RR, 21.981; 95% CI, 3.719–129.924), and inpatient surgery (RR, 8.606; 95% CI, 2.266–32.689). Independent functional status with ADL was protective against surgical complications (RR, 0.023; 95% CI, 0.002–0.221) (Table 4).

30-day general, surgical, and medical measures/complications following procedure
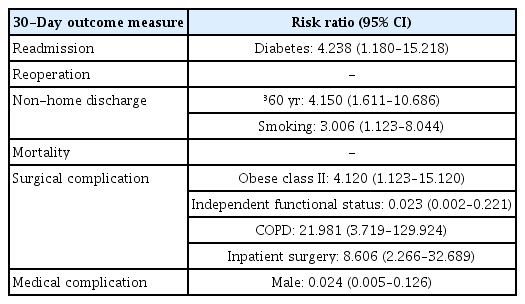
Statistically significant risk factors identified for corresponding 30-day outcome measures/complications
DISCUSSION
The current distal biceps tendon repair literature is limited due to small sample sizes and minimal focus on 30-day complications. Since many of the high-morbidity complications, such as wound infection or emergent reoperation, are likely to occur within several weeks post-surgery, focusing on 30-day complications can help illuminate crucial risk factors. We found readmission, reoperation secondary to distal biceps tendon re-rupture, and non-home discharge to be the most common 30-day complications. Specific risk factors contributing to the short-term complications included diabetes, smoking, female, obesity, COPD, inpatient surgery, and dependent functional status with ADL requiring help from a caretaker. To our knowledge, this is the first study to investigate distal biceps tendon repair complications and related risk factors using the NSQIP database.
Our study found relatively low short-term complication rates compared to related literature. A 2018 retrospective cohort study of 970 distal biceps repair patients found a larger reoperation rate (4.5%) compared to that of the present study (0.6%) [15]. They also found a larger deep infection rate (1.6%) compared to our deep infection rate (0.1%). A recent systematic review found a similar reoperation rate of 1% and a postoperative infection rate of 1.5% compared to the overall postoperative infection rate of 0.4% in our cohort [8]. Although there is a paucity of literature investigating similar complications, this limited comparison suggests lower current short-term complication rates than reported in the literature.
Compared to other types of elbow surgery, distal biceps repair has significantly low complications and risk of re-rupture. A recent systematic review found triceps tendon repair to have a re-rupture rate of 4.62% compared to our re-rupture rate of 0.6% [16]. Another study investigating 417 various elbow arthroscopy procedures observed postoperative superficial infections in 6.7% of cases and a 2.2% postoperation deep infection rate, which is drastically different than our observed 0.2% and 0.1% postoperation superficial and deep infection rate, respectively [17]. Further, studies investigating similar demographic variables as risk factors for complications following triceps tendon repair failed to elucidate any significant risk factors [18]. Based on the available literature, distal biceps repair demonstrates unique outcomes compared to other elbow surgeries, suggesting that distal biceps repair short-term complication risk factors are unique and must be independently investigated, as in this study.
This study demonstrated diabetes (RR, 4.238; 95% CI, 1.180–15.218) to be a risk factor for readmission. Although no studies have investigated diabetes as a risk factor for distal bicep repair short-term complications, animal studies have shown diabetes as a predisposing factor for tendon injuries, and clinical studies have previously associated diabetes with Achilles’ tendinopathy [19,20]. Thus, diabetes can contribute to poor tendon state following surgical repair and an increased chance of readmission. Our study also found smoking (RR, 3.006; 95% CI, 1.123–8.044) and age greater than 60 years (RR, 4.150; 95% CI, 1.611–10.686) to be significant risk factors for non-home discharge. A 2017 study found smoking to be associated with increased re-rupture (odds ratio [OR], 4.86; p=0.423) and combined surgical and clinical failures (OR, 5.64; P=0.091) but found patient age to have no impact on complications [7]. A meta-analysis of a myriad of surgery types found preoperative smoking status to be associated with increased risk of a multitude of postoperative complications including wound complications, general infections, and intensive care unit admission, all of which could contribute to increased non-home discharge rates [21]. Furthermore, smoking has been shown to decrease vascularity in tendons between the proximal and distal blood supply of the distal biceps, which could explain the specific association with distal biceps tendon rupture [22].
We also found obese class II (RR, 4.120; 95% CI, 1.123–15.120) to be a significant risk factor for surgical complications, which agrees with a 2016 study that demonstrated obesity (OR, 1.88; 95% CI, 1.01–3.52) to be associated with adverse postoperative events [9]. Previous literature has found a reduced immune response to acute tendon injury in obese individuals, which might have contributed to our observed increase in surgical complication rate [23]. We could not identify literature related to our findings of dependent function status, COPD, inpatient surgery, and male as risk factors for 30-day complications. However, these novel findings—along with our supported findings of diabetes, smoking, and obesity—can help providers identify patients who could be at greater risk of short-term postoperative complications, especially if a combination of these risk factors is present.
Our study has several limitations that are important to consider when interpreting our findings. First, although our cohort is large relative to that of similar studies, the number of patients with 30-day complications was small. This decreased the statistical power of our study and resulted in large confidence intervals. Congregating a larger dataset containing short-term complications of distal biceps repairs would help address this shortcoming. Second, the NSQIP database has its own unique weaknesses, including a limited number of contributing institutions, especially large teaching hospitals, due to the expensive nature of participation, which can limit the reporting accuracy of the database [24]. Further, the database did not distinguish specific surgical techniques, severity, or time between injury to surgery. Including specific surgical techniques and injury severity could allow determination of additional 30-day complication associations. Finally, our relatively short follow-up duration made it difficult to compare our findings to related studies with longer follow-up and might have resulted in underestimation of short-term complications.
This study contributes to the current body of literature as it is the first to associate several risk factors with 30-day complications in distal biceps tendon repair patients. Large studies have found up to a 25% complication rate, some of which significantly impact patient quality of life [8]. However, there is a lack of short-term complication studies in the literature, which removes focus from the most pressing and severe complications following distal-biceps tendon repair surgery. Our newly identified short-term risk factors will allow providers to inform patients of possible distal biceps repair postoperative risks more accurately and simultaneously take extra precaution when applicable. Future related research including a prospective design, longer follow-up, and a larger sample size would help confirm and explore additional risk factors associated with short-term complications.
Notes
Financial support
None.
Conflict of interest
None.