Primary Total Elbow Replacement for Treatment of Complex Distal Humerus Fracture: Outcomes of Short-term Follow-up
Article information

Abstract
Background
High complication rate after open reduction and internal fixation can lead to use of primary total elbow replacement (TER) in treatment of complex distal humerus fractures in elderly patients. The purpose of this study was to investigate the short-term outcomes and complications after primary TER in patients with complex distal humerus fracture.
Methods
Nine patients with acute complex distal humerus fracture were treated by primary TER using the semiconstrained Coonrad-Morrey prosthesis. The mean age of patients was 72.7 years (range, 63–85 years). Clinical and radiographic outcomes were evaluated over a mean follow-up of 29.0 months (range, 12–65 months) using visual analog scale (VAS) score for pain; Mayo elbow performance score (MEPS); Quick Disabilities of the Arm, Shoulder, and Hand (Quick-DASH) score; and serial plain radiographs. Complications were also evaluated.
Results
At the final follow-up, mean VAS, MEPS, and Quick-DASH scores were 1.2, 80.5, and 20, respectively. The mean range of motion was 127.7º of flexion, 13.8º of extension, 73.3º of pronation, and 74.4º of supination. There was no evidence of bushing wear or high-grade implant loosening on serial plain radiographs. Three complications (33.3%) comprising two periprosthetic fractures and one ulnar neuropathy were observed.
Conclusions
Primary TER for treatment of complex distal humerus fractures in elderly patients yielded satisfactory short-term outcomes. However, surgeons should consider the high complication rate after primary TER.
INTRODUCTION
Distal humerus fractures in the elderly are increasing with the aging population and are difficult to treat and challenging for orthopedic surgeons. The gold standard for treatment of displaced distal humerus fractures is open reduction and internal fixation (ORIF), along with early mobilization [1]. However, these fractures are often complicated by comminution, bone loss, intra-articular involvement, and poor bone quality. Complex distal humerus fractures in elderly patients may have inadequate internal fixation such that bony union is difficult. Successful treatment requires long-term immobilization and produces unsatisfactory clinical outcomes with complications [2]. The complication rate after ORIF for distal humerus fractures has been reported as over 35% [1,2]. The complications include fixation failure, nonunion, heterotopic ossification, ulnar neuropathy, and stiffness [1,2]. These difficulties have led to use of total elbow replacement (TER) as a primary treatment option for complex distal humerus fractures in elderly patients.
Several studies have reported that primary TER produces superior outcomes compared with ORIF and is a reasonable option for elderly patients with comminuted intra-articular distal humerus fractures [3-6]. Over the last decade, the number of displaced distal humerus fractures in elderly patients treated with TER has increased dramatically because of the aging population [7]. The advantages of TER over ORIF include early rehabilitation and satisfactory short-term outcomes. However, the disadvantages include surgeon-imposed activity restrictions and several catastrophic complications including infection, aseptic loosening, periprosthetic fracture, and potential need for revision arthroplasty [8]. With these distinct benefits and risks, it remains unclear whether TER should be a primary treatment of distal humerus fractures in elderly patients. The purpose of this study was to investigate the outcomes and complications after primary TER in patients with complex distal humerus fracture.
METHODS
This study was approved from the Institutional Review Board of Dongsan Medical Center with exemption of informed consent (IRB No. 2019-10-030). Between 2012 and 2019, we treated 16 patients with primary TER for acute complex distal humerus fractures. Nine of 16 patients were retrospectively reviewed because six had died and one was unreachable. Inclusion criteria were (1) age older than 60 years at the time of initial trauma, (2) primary TER for acute fractures, and (3) follow-up period longer than 12 months after surgery. The decision to perform TER was based on patient age and working status, degree of comminution with intra-articular involvement, osteoporosis, and medical comorbidity.
The mean age of the patients was 72.7 years (range, 63–85 years). There were five women and four men. The mechanism of injury was slip in seven patients and fall in two patients. According to AO classification, seven patients had type C3 fracture, one had type A2 fracture, and one had type A3 fracture. One patient had an open fracture. The mean interval from initial trauma to TER was 27.8 days (range, 5–85 days) (Table 1). Three patients underwent temporary external fixation because of one open fracture, one impending compartment syndrome, and one ipsilateral proximal humerus fracture with poor condition of the soft tissue around the elbow joint. One patient with impending compartment syndrome underwent fasciotomy only.
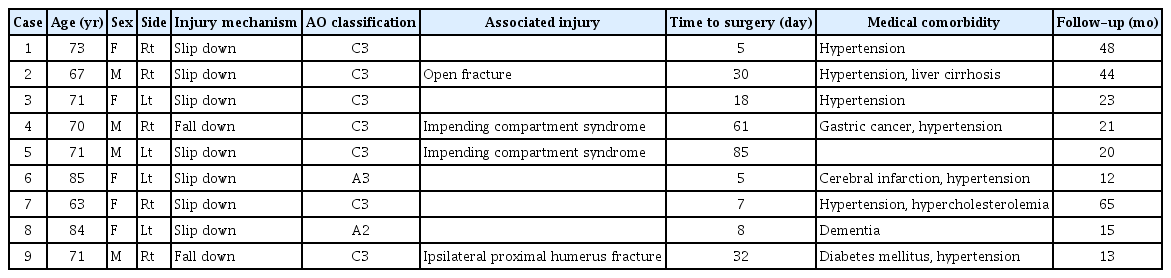
The demographic data of patients
All patients were treated using the semiconstrained Coonrad-Morrey prosthesis (Zimmer, Warsaw, IN, USA) via a triceps reflecting approach, and the ulnar nerve was transposed anteriorly. After surgery, a long-arm splint was applied in full extension to prevent wound perturbation. Passive and active motion exercises were started 2 weeks after surgery.
The mean follow-up period of patients was 29.0 months (range, 12–65 months). Clinical outcomes were assessed using the visual analog scale (VAS) score for pain; Mayo elbow performance score (MEPS); the Quick Disabilities of the Arm, Shoulder, and Hand (Quick-DASH) score; and active range of motion (ROM) of the elbow joint. Serial plain radiographs were performed for all patients to evaluate fixation status, bushing wear, and implant loosening. The cementing technique was evaluated on immediate postoperative radiographs for both components and was classified into three types (adequate, marginal, inadequate) as described by Morrey [9]. Bushing wear was assessed via anteroposterior radiograph at the final follow-up evaluation and was classified into three grades (normal, mild to moderate, extensive) as described by Ramsey et al. [10] Implant loosening was graded on anteroposterior and lateral radiographs according to the classification described by Morrey et al. [9] Radiolucency was graded as type 0 if the radiolucent line was less than 1 mm wide and involved less than 50% of the interface, type 1 if the radiolucent line was at least 1 mm wide and involved less than 50% of the interface, type 2 if the radiolucent line was more than 1 mm wide and involved more than 50% of the interface, type 3 if the radiolucent line was more than 2 mm wide and surrounded the entire interface, and type 4 if there was gross loosening [9].
RESULTS
At the final follow-up evaluation, the mean VAS score for pain was 1.2. Four patients had no pain, four had mild pain, and one had moderate pain. The mean MEPS was 80.5, with two excellent, five good, and two fair results. The mean Q-DASH score was 20. The mean ROM was 127.7º of flexion, 13.8º of extension, 73.3º of pronation, and 74.4º of supination (Table 2).
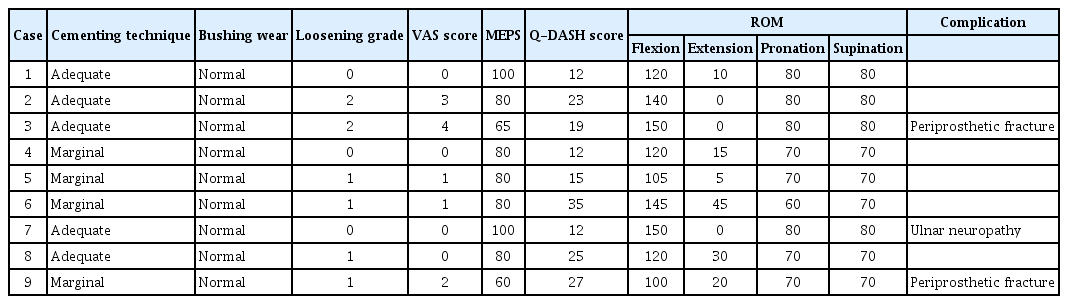
Summary of the outcomes and complication after total elbow replacement in patients with complex distal humerus fracture
For the cement technique on immediate postoperative radiographs, five cases showed adequate adherence, and four cases had marginal adherence. Bushing wear was not observed on the final radiographs in all cases. According to loosening grade, there were three type 0, four type 1, and two type 2 cases on the final radiographs. Three complications (33.3%) were observed in nine patients; two patients with periprosthetic fracture around the humeral component with minor trauma were treated with ORIF and showed fair clinical results at the final follow-up. One patient had progressive ulnar neuropathy after TER and underwent adhesiolysis and decompression of the ulnar nerve at 5 months after TER.
Case 1
A 73-year-old woman (no. 1) was hospitalized for intercondylar comminuted fracture of the right distal humerus after a slip. On the 5th day after injury, we performed primary TER. At 48 months follow-up after TER, the patient had satisfactory clinical outcomes with no evidence of implant loosening (Fig. 1).

(A, B) Initial radiographs and three-dimensional computed tomography images of a 73-year-old woman show an intercondylar comminuted fracture of the right distal humerus. (C) Immediate radiographs after total elbow replacement. (D) Radiographs at 48 months after surgery show no evidence of loosening with excellent clinical outcome.
Case 2
A 63-year-old woman (no. 7) was hospitalized for intra-articular comminuted fracture of the right distal humerus after a slip. On the 7th day after injury, we performed primary TER. After surgery, the patient complained of a tingling sensation of the fourth and fifth fingers. At 5 months after surgery, we performed adhesiolysis and decompression of the ulnar nerve for progressive ulnar neuropathy with clawing deformity. At the 65-month follow-up after TER, the patient had excellent clinical outcomes with no evidence of implant loosening. Ulnar neuropathy was resolved completely (Fig. 2).

(A) Initial radiographs of a 63-year-old woman show a comminuted intra-articular fracture on the right distal humerus. (B) Immediate radiographs after total elbow replacement. (C) Right fourth and fifth finger clawing deformity at 5 months after surgery. (D) Radiographs at 5 months after surgery. (E) Intraoperative findings of adhesion of the ulnar nerve. (F) Radiographs at 65 months after surgery show no evidence of loosening. Clinial photos show full elbow flexion and extension.
DISCUSSION
Although the number of distal humerus fractures in elderly patients has increased in the last decades, the results after ORIF in elderly patients with complex distal humerus fractures are highly variable, with many failures and poor outcomes [3-6]. Originally, TER was restricted to manage rheumatoid arthritis, posttraumatic arthritis, and fracture nonunion of the distal humerus. Recent studies have reported that primary TER for complex distal humerus fractures in elderly patients may be an alternative treatment with satisfactory outcomes [11-14]. TER involves immediate stability, early mobilization, faster rehabilitation, and better short-term functional result in older low-demand patients with osteoporosis [4]. However, TER may accompany considerable postoperative complications such as infection, implant loosening, neurological problems, and periprosthetic fracture.
Several studies have reported short- to long-term outcomes and complication rate after TER for complex distal humerus fractures [5,6,11,12,14]. In 1997, Cobb and Morrey [12] first reported a series of 21 elderly patients who underwent primary TER for comminuted distal humerus fractures. They reported good or excellent results in 95% of patients at a mean follow-up of 3.3 years, with a reoperation rate of 5%. Lami et al. [14] reported 21 patients receiving TER for distal humerus fractures with a mean follow-up of 3.2 years, mean MEPS of 84, Q-DASH score of 32.4, mean flexion of 125º, and mean loss of extension of 22º. The complication rate was 9.5% without any revision surgery. Lee et al. [5] reported seven elderly Asian patients with distal humerus fractures treated with TER and achieved six excellent results and one good result in patients with low physical demands. The mean MEPS was 94.3 points, and mean follow-up was 24.9 months. Barco et al. [11] reported 44 TER in treatment of distal humerus fracture; patients were followed for a minimum of 10 years. The mean VAS for pain was 0.6, the mean flexion was 123º, and mean loss of extension was 24º. The mean MEPS was 90.5 points, with three patients scoring <75 points.
Mckee et al. [2] conducted a prospective, randomized, controlled trial to compare functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular distal humeral fractures treated with ORIF or primary semi-constrained TER. They reported that TER resulted in more predictable and improved 2-year functional outcomes compared with ORIF and may result in decreased reoperation rates (12% in TER group vs. 29% in ORIF group) [2]. Five patients randomized to ORIF were converted to TER intraoperatively because of extensive comminution and inability to obtain sufficient stability to allow early ROM [2]. Frankle et al. [3] conducted a retrospective comparison of ORIF with TER for intra-articular distal humerus fractures in 24 women aged older than 65 years. At a minimum of 2 years, TER resulted in excellent or good results in all 12 patients, with improved ROM and less physical therapy required compared with an ORIF group. Federer et al. [13] investigated total cost and effectiveness of TER compared to ORIF and reported that TER was slightly more cost effective than ORIF in elderly patients with acute intra-articular distal humerus fractures. In a systematic review by Githens et al. [8], 27 studies with 563 patients showed a mean follow-up after TER of 45.9 months, whereas follow-up after ORIF was 43 months. That group reported no clinically evident difference in functional outcomes as measured by ROM and functional scores [8]. Although total complications were more frequent after TER, major complications were more frequent after ORIF [8]. However, the study quality in that systematic review was generally weak. Because the optimal treatment for complex distal humerus fractures has not yet established, further prospective randomized trials are needed to assess and determine the most appropriate surgical intervention for complex distal humerus fracture.
A systematic review article by Chalidis et al. [4] reported nine clinical studies describing the results and complications of TER in 167 patients with 169 distal humerus fractures. Complications included wound infection (5.4%), ulnar nerve lesion (6.5%), reflex sympathetic dystrophy (3%), and periprosthetic fracture (1.7%). Barco et al. [11] reported a 92% survival rate for elbows without rheumatoid arthritis at both 5 and 10 years, but complication was frequent; 23 events (52%) were observed in 44 patients. Prasad and Dent [6] reported their experience of 19 TER for distal humerus fracture with a minimum 10-year follow-up. Only 53% of nonrheumatoid patients who undergo TER for distal humerus fractures survive to the 10th anniversary of their index procedure. They concluded that surgeons undertaking these procedures should be aware of the long-term revision rates and the sex difference in rates of loosening [6].
In the present study, mean VAS score, MEPS, and Quick-DASH at the mean follow-up of 29 months were 1.2, 80.5, and 20, respectively. The mean ROM was 127.7º of flexion, 13.8º of extension, 73.3º of pronation, and 74.4º of supination. Moreover, there was no evidence of bushing wear or high-grade implant loosening on serial plain radiographs. Our study demonstrated that primary TER produces satisfactory short-term functional and radiographic outcomes in patients with complex distal humerus fractures. However, we detected three complications (33.3%) in nine cases, including two periprosthetic fractures and one ulnar neuropathy that required secondary operation. The patient with progressive ulnar neuropathy recovered completely after adhesiolysis and decompression of the ulnar nerve at 5 months after TER, but two patients with periprosthetic fracture were treated with ORIF and showed unsatisfactory clinical outcomes at the final follow-up. In terms of TER indication, primary TER for complex distal humerus fractures should be selected carefully based on patient age, bone quality, comorbidities, soft tissue condition, and intra-articular comminution because of potentially considerable postoperative complications.
This study has several limitations. First, it was a retrospective study with a small number of cases. Second, the results may not be generalizable because seven (43.7%) of 16 patients died or were lost during follow-up. Third, the follow-up period was relatively short and did not allow exact radiographic results including bushing wear or implant loosening in long-term implant survival. In the future, long-term prospective studies are needed to evaluate clinical and radiographic outcomes after TER for complex distal humerus fractures.
This study revealed that primary TER for treatment of complex distal humerus fractures in elderly patients yielded satisfactory short-term outcomes. However, surgeons should consider the high complication rate after primary TER.
Notes
Financial support
None.
Conflict of interest
None.