Histological Changes in Biceps Muscle after Tenotomizing the Biceps Long Head in a Rat Model
Article information

Abstract
Background
Popeye deformity is common after rupture of the biceps muscle’s long head tendon. Herein, we report on histological changes in biceps brachii muscles following tenotomy of the long head biceps tendon.
Methods
Twelve Sprague-Dawley rats (12-week-old) underwent tenotomy of the long head biceps tendon in the right shoulder. At postoperative weeks 4, 7, and 10, the operative shoulders were removed by detaching the biceps brachii muscle from the glenoid scapula and humerus; the opposite shoulders were removed as controls. H&E staining was performed to elucidate histological changes in myocytes. Oil-red O staining was performed to determine fatty infiltration. Myostatin antibody immunohistochemistry staining was performed as myostatin is expressed by skeletal muscle cells during myogenesis.
Results
H&E staining results revealed no changes in muscle cell nuclei. There were no adipocytes detected. Compared with that of the control biceps, the cross-sectional area of the long head biceps was significantly smaller (p=0.00). Statistical changes in the total extent of the 100 muscle cells were significant (p=0.00). Oil-red O staining revealed no fatty infiltration. Myostatin antibody immunohistochemical staining revealed no significant difference between the two sides.
Conclusions
Muscular changes after tenotomy of the long head biceps included a decrease in the size of the individual muscle cells and in relative muscle mass. There were no changes observed in muscle cell nuclei and no fatty infiltration. Moreover, there were no changes detected by myostatin antibody immunohistochemistry assay.
Introduction
Shoulder pain is a common medical problem and may lead to an inability to carry out daily living-activities. Luime et al. [1] reported that shoulder pain was present in approximately 14.7 persons per 1,000 persons per year in a primary care unit, whereas lifetime prevalence of shoulder pain was approximately 70% of the general population. In that review, the most common reported cause of shoulder pain was rotator cuff disease [1].
Due to its anatomical location and its long, oblique course in the shoulder joint, the biceps long head tendon is a frequent source of disorders associated with other shoulder pathologies, especially rotator cuff tear [2,3]. Murthi et al. [4] reported that the incidence of biceps pathology in patients is as high as 63% with rotator cuff disease, and Chen et al. [5] reported that a normal biceps long head tendon is observed in only 24% of patients with rotator cuff tears. Alpantaki et al. [6] identified sympathetic and sensory neural elements in the long head biceps tendon by applying immunohistochemical stains and indicated that those elements act as a major source of shoulder pain. Some studies have suggested that the outcome of a rotator cuff repair can be compromised if a concomitant biceps lesion is left untreated [7,8].
Problems associated with the biceps long head tendon may be placed in four groups. The first includes tenosynovitis and tendinitis due to degeneration of the tendon; the second involves tendon rupture caused by the progressive development of tendinitis; the third includes instability and dislocation caused by failure of the stabilizing process of the biceps pulley; the fourth and final problem involves rupture of the insertional portion of the tendon, often occurring in relatively young patients and/or those involved in sports activities.
The so-called Popeye deformity can be caused by distal movement of the ruptured biceps long head tendon. There were several reports indicating that the Popeye deformity produces cosmetic complaints, cramping, spasmodic pain, reduction of elbow flexion powers, and supination of the forearm [9-11]. However, there are no known reports on the pathogenesis of symptoms and histological changes that occur following the development of a Popeye deformity.
Research into the degeneration of the muscles of the shoulder has primarily focused on atrophy and fatty infiltration of the supraspinatus and infraspinatus muscles associated with chronic, massive rotator cuff tears. Moreover, there are reports that previously developed fatty infiltrations were irreversible even though the massive rotator cuff tear was repaired [12,13]. Previous research into the biceps long head tendon has been primarily related to describing specific techniques for surgical treatment and presenting subjective outcomes of patients after treatment. Unfortunately, there is an absence of reports on differences between such surgeries and describing good and bad clinical outcomes in patients.
Thus, the authors formed a hypothesis that atrophy and fatty infiltration occur after rupture of the biceps long head tendon. To investigate that hypothesis, we established a Popeye deformity animal model and evaluated the histological changes in muscle cells after tenotomy of the biceps long head tendon in the rat model.
Methods
The study was approved by the Institutional Animal Care and Use Committee of The Catholic University of Korea (No. PSPH-20130923-01).
Experimental Subjects and Procedure
The animal experiments were performed on 12-week-old Sprague-Dawley rats. The study was designed to compare histological differences in the biceps muscle cells of groups of rats at 4, 7, and 10 weeks after tenotomy of biceps long head tendon. The 4-, 7-, and 10-week assessment groups were each assigned four rats. For all rats, the right shoulder was set as the experimental side and the left shoulder was set as the control side.
Surgical Technique
After inhalation-based anesthesia, a longitudinal skin incision was made along the long axis of the humerus and the biceps long head tendon was exposed at the bicipital groove while preserving the deltoid muscle. Tenotomy was performed at the proximal level of the bicipital groove (Fig. 1). After identification of the retracted stump at the distal cutting edge, the skin incision was closed and sutured. Gentamicin (5 mg/kg) and ketoprofen (5 mg/kg) were administered as a prophylactic antibiotic and for postoperative pain control, respectively.
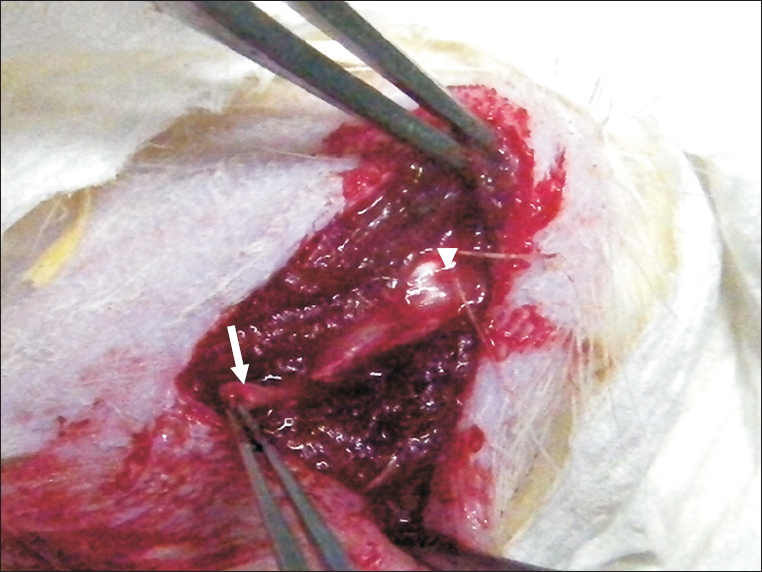
Image showing tenotomized biceps long head tendon (arrow) at the bicipital groove (arrowhead) of a rat.
After the surgery, rats were maintained without constraints in a cage. At 4, 7, and 10 weeks after the operation, a group of four rats was euthanatized, and their tenotomized biceps muscles, as well as the associated tendons, were removed. The biceps muscle from the opposite side was removed in the same manner and acted as the control sample. After being fixed in 10% formalin (pH 7.4) for 12 hours, muscle tissue was separated from the other biceps tissues.
Histological Examination
Following tissue sample dehydration using 10% formalin, muscle tissue samples were embedded in a paraffin block. Sections were obtained and were subjected to H&E staining to observe histological changes to myocytes or underwent Oil-red O staining to identify fatty infiltration. Immunohistochemical staining for myostatin, which acts as a growth differentiation factor, was also performed. The myostatin activity level is reduced when muscular atrophy has occurred.
Measurement of Cross-sectional Area
For this analysis, cross-section muscle samples were examined under a microscope (Olympus DP 70; Olympus, Tokyo, Japan) and analyzed by using Toupview software (ToupTek, Hangzhou, China). The cross-sectional area of 100 muscle cells was calculated by using Image J program (National Institutes of Health, Bethesda, MD, USA). To compare the muscle cell cross-sectional areas of the experimental and control groups, the sums of the cross-sectional areas of 100 muscle cells in the biceps long head and biceps short head of the two groups were determined (Fig. 2). The ratios of the cross-sectional areas in the short head biceps and the long head biceps of the two groups were calculated. All areas were calculated in pixel units.
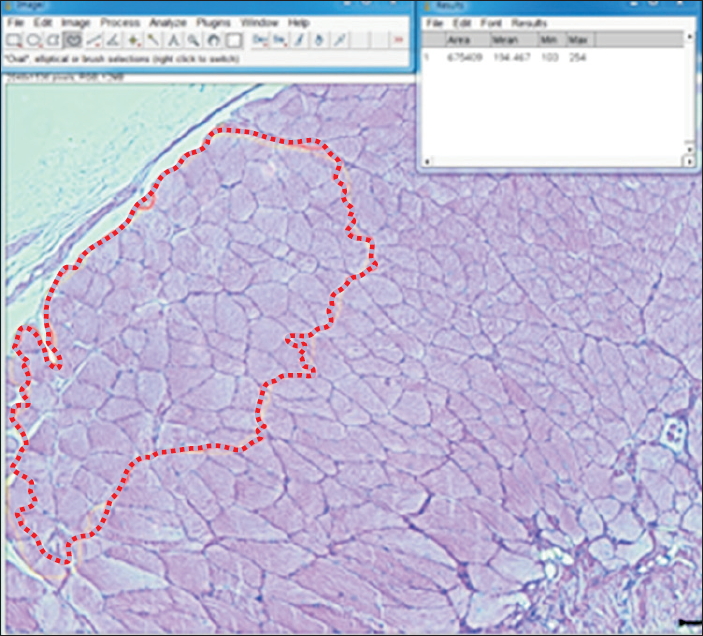
Screen capture of Image J program showing microscope-based measurement of biceps muscle cross-sectional area. The area within the bold dotted line includes 100 muscle cells.
Statistical Analysis
Statistical analyses were performed by using SPSS Statistics software ver. 12.0 (SPSS Inc., Chicago, IL, USA), and the statistical significance level was set at 95%. The Student’s t-test and one-way ANOVA were used. In addition, the non-parametric Wilcoxon signed rank, Kruskal-Wallis, and Mann-Whitney tests were used.
Results
Gross Observations
All right-shoulder, experimental sides revealed retraction of the biceps long head tendon, distal movement of the central portion of the biceps muscle, and hypertrophy (Fig. 3).
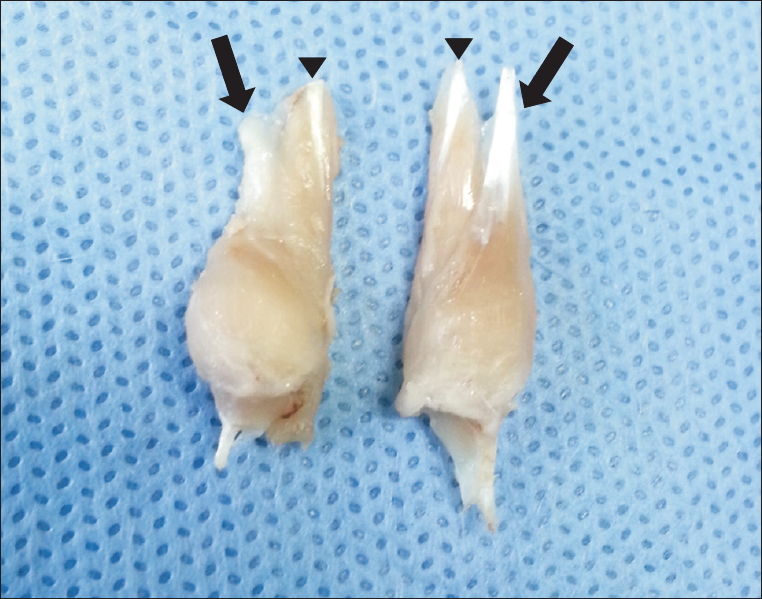
Popeye deformity of biceps muscle after tenotomy (left) and a normal appearing biceps muscle (right) (arrows: biceps long head tendon, arrowheads: biceps short head tendon).
H&E Stain Results
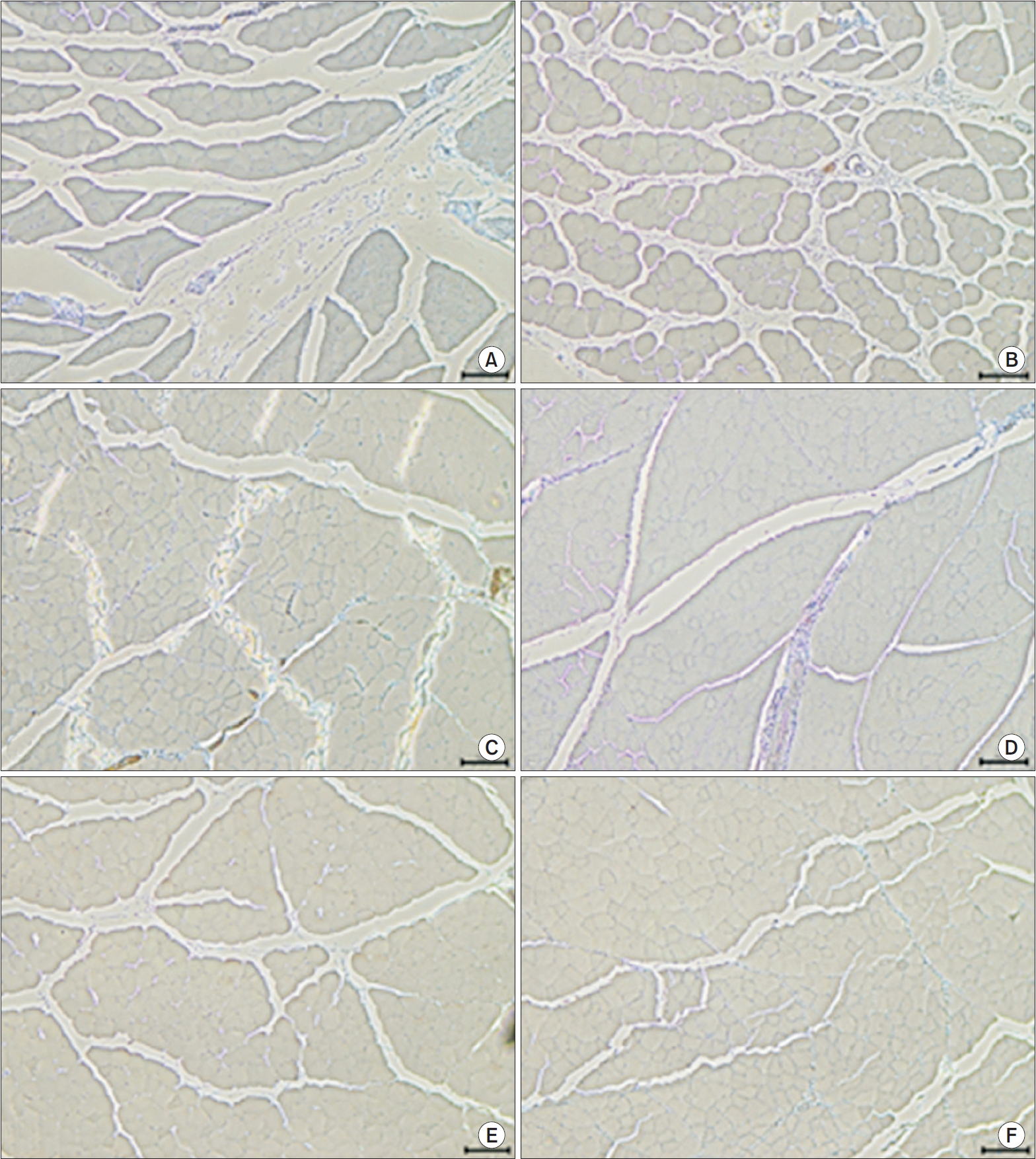
The H&E staining results revealed an absence of adipocytes and no morphological changes in the nuclei of the muscle cells on the experimental side (Fig. 4).
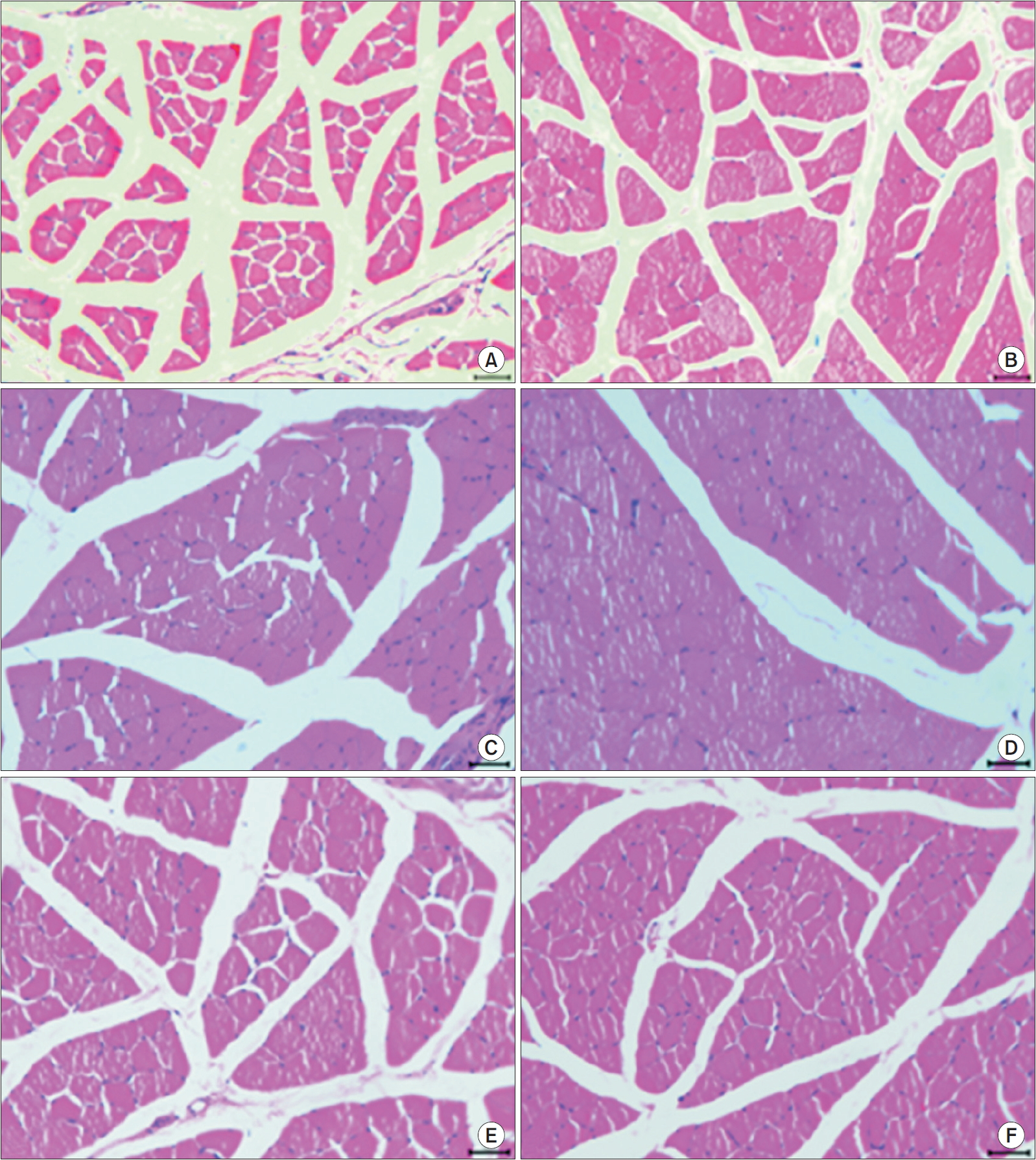
H&E staining of biceps muscles from experimental and control shoulders (×200). (A) Experimental shoulder at 4 weeks after surgery. (B) Control shoulder at 4 weeks after surgery. (C) Experimental shoulder at 7 weeks after surgery. (D) Control shoulder at 7 weeks after surgery. (E) Experimental shoulder at 10 weeks after surgery. (F) Control shoulder at 10 weeks after surgery.
Oil-red O Stain Results
The Oil-red O staining did not reveal fatty infiltration and no adipocytes were observed on the experimental side (Fig. 5).

Oil-red O staining of biceps muscles from experimental and control shoulders (×200). (A) Experimental shoulder at 4 weeks after surgery. (B) Control shoulder at 4 weeks after surgery. (C) Experimental shoulder at 7 weeks after surgery. (D) Control shoulder at 7 weeks after surgery. (E) Experimental shoulder at 10 weeks after surgery. (F) Control shoulder at 10 weeks after surgery.
Myostatin Immunohistochemical Stain Results
The myostatin staining results showed no significant difference in myostatin presence between the right-shoulder experimental side and the left-shoulder control side (Fig. 6).
Myostatin immunohistochemical staining of biceps muscles from experimental and control shoulders (×100). (A) Experimental shoulder at 4 weeks after surgery. (B) Control shoulder at 4 weeks after surgery. (C) Experimental shoulder at 7 weeks after surgery. (D) Control shoulder at 7 weeks after surgery. (E) Experimental shoulder at 10 weeks after surgery. (F) Control shoulder at 10 weeks after surgery.
Cross-sectional Areas
The ratios of the cross-sectional area of 100 muscle cells in the biceps long head to that in the biceps short head on the right (experimental) and left (control) sides were determined. Student’s t-test results indicated a significantly low ratio on the experimental side than that on the control side (p=0.00). Similar results were obtained when the non-parametric Wilcoxon signed rank test was applied (p=0.02). The non-parametric Kruskal-Wallis test also showed a lower ratio on the experimental side, but the difference between the two sides was not significant (p=0.06). The non-parametric Mann-Whitney test showed significantly lower ratios on the experimental side than on the control side at 4, 7, and 10 weeks after surgery (p=0.043). All rats in the 4-, 7-, and 10-week assessment groups had lower biceps long head cross-sectional areas than biceps short head cross-sectional areas on the tenotomized side (Fig. 7).
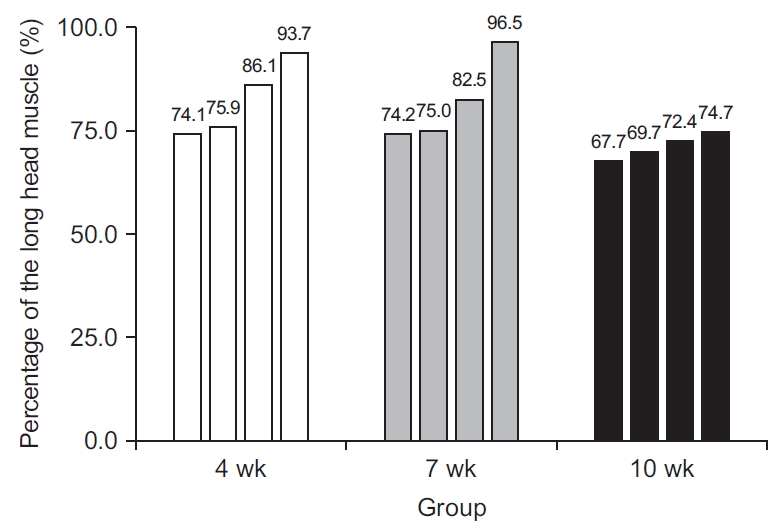
Graph showing the percentage of 100 myocytes of the biceps long head muscle compared to 100 myocytes in the biceps short head muscle for each rat in each of the assessment week groups.
Compared to the control side, the ratio of the cross-sectional area of the biceps long head and that of the biceps short head was significantly lower on the experimental side (based on paired Student’s t-test and Wilcoxon signed rank test results (p=0.00).
Discussion
Interestingly, muscle atrophy and fatty infiltration following the tenotomizing of the biceps long head tendon, which were hypothesized for this study, were not observed. However, all rats that underwent the tenotomy grossly exhibited the Popeye deformity.
The biceps brachii muscle has two origins; the short head originates from the coracoid process and the long head originates from the supraglenoid tubercle and glenoid labrum [3]. Due to its anatomical location and pathway, damage to the biceps long head tendon can induce shoulder problems, especially when accompanied by rotator cuff tear, resulting in long-term shoulder pain. It has been reported that the long head tendon prevents superior and anterior displacement of the humeral head, but that remains controversial. The occurrence of the Popeye deformity after a biceps long head tendon tear is reported to occur in 3% to 63% of cases [14-16], and prevalence of the Popeye deformity after failed fixation of biceps long head tears is approximately 2% [17]. With the Popeye deformity, symptoms such as weakened elbow flexion and forearm supination may occur. Moreover, there are many Popeye deformity patients that have complained of spastic pain [9-11], but the pathogenesis of that pain has not been fully described.
Muscle contraction followed by tearing of the biceps long head can be diagnosed grossly (e.g., the Popeye deformity) by identifying a mass-like lesion caused by the contracted muscle on the anteromedial aspect of the humerus. Ultrasonographically, the biceps long head tendon appears homogeneously hyperechoic, similar to normal tendons, and longitudinal long collagen fibers are visible. However, a contracted tendon appears unevenly hypoechoic with its collagen fibers showing an irregular pattern. The distal part of a torn biceps long head may be located distal to the biceps groove. Moreover, magnetic resonance imaging (MRI) of a torn biceps long head tendon may show absence of a portion of that tendon from its typical location, known as the ‘empty groove sign’, and retraction and atrophic changes to the distal part of the torn tendon can be seen [18,19].
Generally, atrophic changes to and fatty infiltration of the muscle occur after chronic, massive rotator cuff tears. These features are detectable through computed tomography, MRI, and/or pathologic results. However, such fatty infiltration does not reduce after repair of a torn rotator cuff [12,13,20,21].
In this study, an animal model was established by inducing biceps muscle retraction after tenotomy of the biceps long head tendon of rat. In that model, postoperative fatty infiltration, which is seen after a rotator cuff tear, was not observed. Since the biceps is formed of long head and short head branches, it is speculated that, after tenotomy of the long head branch, the short head branch was able to compensate and provide whole muscle reactions, thereby preventing fatty infiltration. Further investigation of that speculation is needed.
The rat Popeye deformity animal model is deemed to be successfully established because all rats undergoing tenotomy in this study showed the Popeye deformity. However, some human cases with biceps tendon damage do not show the Popeye’s deformity due to auto-tenodesis. In the rat model, retraction of the cut tendon end beyond the bicipital groove can be confirmed under direct vision. That creates a notable difference between some human clinical cases and the rat model.
The results of this study are important as this is the first study reporting muscle atrophy pathologically by showing reduced sizes of individual muscle cells and a reduced cross-sectional area of the long head muscle portion compared to that of the short head portion. This size difference could be a basis for using tenodesis to treat a biceps long head tear, which is still controversial between tenodesis and tenotomy. Surgeons who prefer tenotomy over tenodesis suggest that the clinical outcome of tenotomy is satisfactory [15,22,23], and that not all of their patients show the Popeye deformity. They support their assertions by suggesting the presence of autotenodesis of the biceps long head at the biceps groove; however, autotenodesis does not occur in all cases [24].
The limitations of this study are that although muscle cell size was affected, histologic changes after tenodesis were not detected; thus, further study is needed. Second, the absence of fatty infiltration, which was one of the hypotheses of this study, might have been caused by damage to fatty tissue during tissue dehydration in the process of placing samples in paraffin blocks. However, if there were dehydrated fat tissues present there should be empty spaces observed between muscle cells, and no such spaces were seen in the H&E stained sections. Therefore, we concluded there was no fatty infiltration.
Conclusion
Muscular changes after tenotomy of the biceps long head tendon include decreases in the size of individual muscle cells and a decrease in relative muscle mass. There were no posttenotomy changes in muscle cell nuclei and no evidence of fatty infiltration. Moreover, there were no changes observed following myostatin antibody immunohistochemical staining.
Notes
Research Ethics
IACUC approval: The Catholic University of Korea (No. PSPH-20130923-01).
Financial support
None.
Conflict of interest
None.