Arthroscopic Capsular Repair without Relaying Sutures: ‘Simple Sewing Technique’
Article information

Abstract
We report a simple technique for repairing capsular tear, using only a hook-like, cannulated instrument and braided sutures without relaying steps. A No. 2 braided suture is passed through the lumen of the instrument. Under direct arthroscopic view, the tip of the instrument is passed through the side of the capsule that has previously been separated with the probe. One end of the suture is retrieved with a grasper through a separate portal. The tip is moved back without withdrawing through the skin, and reinserted into the other side of the capsule. Holding the end retrieved earlier, the other end of the suture is retrieved with a suture retriever. After complete removal of the instrument, the suture is tied through a cannula using the standard knot tying techniques. The same procedures are repeated for other required knots.
Introduction
To enable a capsule-to-capsule repair during arthroscopic procedures, hook-type instruments can be used to pass a monofilament suture (e.g., polydioxanone [PDS], nylon) or wire-loop (e.g., Shuttle RelayTM; Conmed Linvatec, Largo, FL, USA). Subsequently, these instruments can be used to relay a non-absorbable braided suture. However, positioning of portals at an acute angle could result in tearing of the thin tissue during relaying.
Some surgeons prefer using an absorbable monofilament suture to repair the capsule, which results in a larger knot, thereby causing irritation or synovitis until the monofilament suture is resorbed. Braided sutures are preferred to prevent slippage of knots since friction created is greater for knots tied with braided multi-filament sutures than with monofilament sutures [1].
In this paper, we report a simple technique for repairing capsule-to-capsule, using braided sutures without relaying steps. Since this technique requires simple back and forth needle movements, similar to a sewing machine, we have termed it the ‘simple sewing technique’.
Technique
Conventional repair of torn capsules encountered during arthroscopic procedures can be accomplished using hook-like instruments, cannulas and relaying of sutures. However, if conventional techniques are not possible due to the requirement of an acute angle, or concerns over shuttling of sutures through the thin tissue, the repair can be achieved using the simple sewing technique.
Briefly, a probe is used to separate the torn capsular free ends as much as possible from the overlying rotator cuff tissue. This prevents the attachment of any unwanted tissue to the capsule within the knots.
After assessing the surface anatomy, the optimal entry point for the cannulated instrument (e.g., SutureLasso; Arthrex, Naples, FL, USA) is identified, ensuring that it minimizes the risk of damaging important neurovascular structures. A spinal needle is first inserted into the joint through the gap between the torn capsular flaps. After identifying the appropriate entry point and angle, the needle is removed and a small stab incision is made. A No. 2 braided suture (Fiberwire; Arthrex) is passed through the lumen of the instrument. The portion of the suture end protruding through the tip of the instrument is folded back on itself over the bevel of the tip. During the remainder of the procedure, ensure facing bevel of the tip to the suture, to prevent damaging the suture by the sharp tip. The tip with the suture folded over its bevel is inserted into the joint through the torn gap of the previously made stab incision (Fig. 1A). The tip is subsequently retracted back. Under direct arthroscopic view, the tip is passed through the capsule that was previously separated with the probe (Fig. 1B). One end of the suture is retrieved with a grasper through a separate portal (Fig. 1C). The tip is moved back without withdrawing through the skin, and is reinserted into the other side of the capsule (Fig. 1D). Firmly holding the end retrieved earlier, the other end of the suture is retrieved using a suture retriever (Fig. 1E). After complete removal of the instrument (Fig. 1F), the suture is tied through a cannula using standard arthroscopic knot tying techniques. The same procedures are repeated for subsequent knots, if required.

Schematic drawings showing the ‘simple sewing technique’. (A) Insertion of a hook-like instrument (SutureLasso; Arthrex, Naples, FL, USA) through the torn gap. (B) Passage of the tip through one side of the capsule. (C) Use of a grasper to retrieve one end of the suture from another portal. (D) Movement of the tip and passage through the opposite side under arthroscopic view. (E) Retrieval of the suture using a suture retriever. (F) After complete removal of the instrument, the suture is tied with routine knot methods through a cannula.
Discussion
In arthroscopic procedures, sutures are often passed through soft tissues in a narrow joint space, and torn capsules may be encountered in unstable glenohumeral joints. In addition, multidirectional instability may require rotator interval closure or capsular plication. During arthroscopy of the elbow or knee, it is also possible to encounter capsule or soft tissues that require repair.
To enable these procedures, curved, cannulate, hook-like devices (e.g., Spectrum; Conmed Linvatec and SutureLasso; Arthrex) can be passed through a monofilament or wire loop (e.g., Shuttle RelayTM) through the tissue (Fig. 2). This is followed by tying the monofilament suture, or switching to a braided suture using the relaying technique. During the suture-relaying step of capsular repair, the capsular tissue may be severed. This may occur if the angle of relaying path is acute.
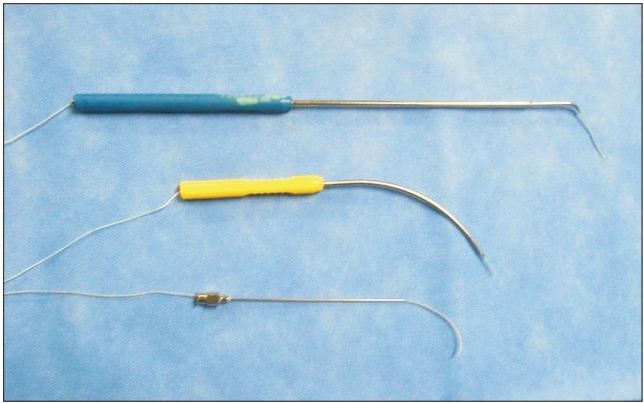
Photographs showing braided sutures (No. 2 Fiberwire; Arthrex, Naples, FL, USA) passed through a SutureLasso (Arthrex) (upper), Banana Lasso (middle), and 18G spinal needle (lower).
A suture could be passed through both sides of a capsule through the cannula located just external to the capsule, and tied blindly outside the capsule. However, this blind knotting may encompass some unwanted tissue, and also fail to produce a properly secure knot. Furthermore, inserting other knots would be difficult under these circumstances. Thus, tying a knot under arthroscopic view may provide better security.
Halbrecht [2] reported the all-inside patellar realignment technique using a spinal needle and PDS suture. However, he passed the stiffer absorbable suture through the needle after penetrating the soft tissue. Relaying steps for non-absorbable, braided suture are required when applying his technique.
Percutaneous use of a hook-like instrument to pass the suture may be more desirable than using a cannula for knotting or skin incision with a scalpel, as it contributes to lesser soft tissue damage. The strength of the specialized braided suture usually allows passage of the needle twice, without removing the suture. This facilitates placing the suture with both free ends within the joint space, and enables it to be tied under direct visualization. However, the No. 2 braided suture routinely used cannot be passed through some hooks (e.g., Spectrum).
We believe that this technique could also help simplify other procedures that pass sutures through soft tissue. These include labral repair using knotless anchors [3,4] and side-to-side sutures of cuff tears [5]. Furthermore, this technique can be applied for capsular placation, portal closure (Fig. 3), rotator interval closure [6], and other surgical methods.

Arthroscopic photo showing portal closure.
Notes
Research Ethics
IRB approval: The Catholic University of Korea, St. Paul’s Hospital (No. PC19RESI0080).
Conflict of interest
None.
Financial support
None.