INTRODUCTION
In shoulders with rotator cuff deficiencies, humeral head (HH) decentralization appears as a superior migration [1,2]. There have been numerous reports on the clinical implications of superior HH migration in patients with rotator cuff tear (RCT) and its correlation with clinical outcomes following arthroscopic rotator cuff repair (ARCR) [3-7]. Chalmers et al. [3] reported that proximal humeral migration occurred in patients with large RCT and infraspinatus involvement over a median follow-up period of 8 years. A study by Kuptniratsaikul et al. [4] found that superior HH migration correlated with arthroscopic reparability of large-to-massive RCTs.
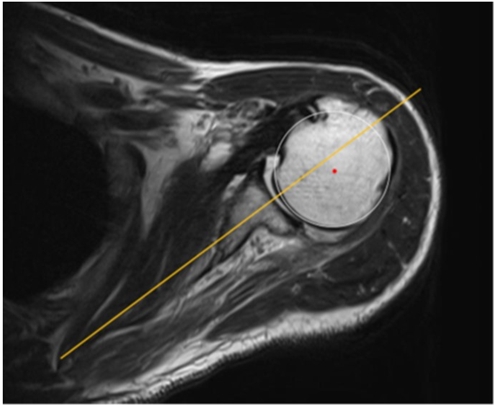
Contrastingly, we occasionally observed subtle posterior HH migration in the glenoid fossa with RCT on axial magnetic resonance imaging (MRI) (Fig. 1). Considering the posterior HH subluxation and posterior glenoid wear that occurs in patients with cuff tear arthropathy, it is understandable that subtle posterior decentering (PD) of the HH can occur from rotator cuff deficiency. Although posterior subluxation is frequently reported in degenerative joint disease, there are few reports on PD in RCT without degenerative change [8,9]. Yun et al. [8] reported that PD detected on MRI arthrography was significantly associated with posterior synovial proliferation and rotator cuff atrophy. Kim and Seo [9] found that PD occurrence was related to tear size and fatty degeneration (FD) of the rotator cuff.
However, little is known about the effect of PD following RCT treatment. This study aimed to investigate the correlation between PD and retear after ARCR. We hypothesized that posterior HH decentering is correlated with retear after ARCR.
METHODS
This retrospective study was approved by Institutional Review Board of Kurume University (IRB No. 19072), and informed consent was obtained from patients. We identified all patients from a surgical registry with a minimum follow-up period of 12 months who underwent complete ARCR between January 2016 and December 2017 at our institution and who underwent both pre- and postoperative MRI evaluations. Patients who underwent partial repair or revision surgery were excluded.
Surgical Technique
The patients underwent ARCR in the beach-chair position under general anesthesia along with an interscalene block. Diagnostic arthroscopy was performed, and tear size was evaluated according to the DeOrio and Cofield classification [10]. Subsequently, the torn tendon was repaired using the single-row repair or double-row suture bridge techniques depending on tendon mobility and tear configuration. For single-row repairs, one row of anchors was placed on the lateral aspect of the rotator cuff footprint, and the torn cuff was fixed with an interrupted suture. For double-row suture bridge repairs, one row of anchors was placed on the medial aspect of the rotator cuff footprint with or without tying, and the torn cuff was transosseously fixed with a knotless anchor on the lateral aspect of the rotator cuff footprint. If needed, additional procedures including capsular release, tenotomy or tenodesis of the long head of the biceps tendon (LHB), distal clavicle excision, and arthroscopic subacromial decompression were performed. Particularly, partial repair was chosen when over-tensioning was required to move the tendon edge to a position just lateral to the articular margin, even after peritendinous adhesions and capsular contractures were released and any interval slides were performed [11,12].
Rehabilitation Protocol
Postoperatively, patients were immobilized using a sling with an abduction pillow, with the shoulder internally rotated at 30°–40° and abducted at 20°. Passive shoulder range of motion (ROM) exercises were commenced on postoperative day 4, and active ROM exercises were allowed at postoperative week 6. Isotonic muscle strengthening exercises were allowed at postoperative week 12 [11,12].
Clinical Assessment
Clinical outcomes were assessed using the Japanese Orthopaedic Association (JOA) and University of California, Los Angeles (UCLA) scores. Physical examinations were performed by an independent physical therapist who was blinded to the study. The outcome measures were assessed preoperatively and at final follow-up.
Structural Assessment
According to the arthroscopic findings, tear morphology (anterosuperior tear/posterosuperior tear/others) and LHB pathology (intact LHB/injured LHB/absent LHB) were analyzed [13]. The radiographic outcome was evaluated according to the Hamada classification on standard anteroposterior shoulder radiographs prior to surgical treatment [14].
All patients underwent MRI preoperatively and at final follow-up. All imaging was performed on a 1.5-Tesla scanner (Excelart; Toshiba Medical Systems, Tokyo, Japan) using routine pulse sequences with the patient in the supine position and the arm in a neutral position. The scans were reviewed by experienced orthopedic doctors who were blinded to this study.
When a fluid-equivalent signal was found or when there was non-visualization of the rotator cuff tendon on more than one T2-weighted image, a retear was diagnosed at final follow-up [15]. FD of the subscapularis (SSc), supraspinatus (SSp), and infraspinatus (ISp) muscles was preoperatively evaluated on the most lateral oblique sagittal T2-weighted MRI that visualized the scapular spine in contact with the scapular body (the “Y-view”), using the Goutallier classification system [16].
PD was evaluated on pre- and postoperative MRI scans. We used T2-weighted axial images at the mid-glenoid level. The transverse axis of the scapula was detected as a line drawn from the medial end of the scapula to the mid-point of the glenoid fossa. PD was confirmed as present if the center of the HH had shifted more than 2 mm posterior to the scapula (Fig. 2) [8,9]. To assess the reproducibility, a random sample of 30 axial MRI slices from 30 individuals was reviewed twice by two observers (KE and YN) who were blinded to the study.
Statistical Analysis
Statistical analysis was performed using JMP 14 (SAS Institute, Cary, NC, USA). For all calculations, the level of significance was defined as p<0.05. Data are expressed as mean value with standard deviation. The Mann-Whitney U-test was used to compare the pre- and postoperative clinical outcomes. The chi-square test was used to compare the nominal variables (retear, DeOrio and Cofield classification, Goutallier classification, and PD) in the structural outcomes. Intra- and interobserver agreement for the PD analysis were evaluated using the Cohen κ statistic and divided into the following categories: very good (0.81–1.00), good (0.61–0.80), moderate (0.41–0.60), fair (0.21–0.40), or poor (0.00–0.20) [17].
RESULTS
There were 162 RCT patients who underwent ARCR at our institution from January 2016 to December 2017. Among these patients, 135 shoulders of 132 patients were enrolled in this study. The remaining 30 patients were excluded, including 2, 11, and 17 who underwent revision surgeries, partial repairs, or who were not followed up for at least 1 year, respectively.
Among the 135 shoulders of the 132 patients included, the mean age at the time of surgery was 63.7±10.3 years (range, 30–88 years). The mean symptom duration preoperatively was 8.4±7.9 months (range, 1–48 months). Single-row repairs were performed in 22 shoulders (16.3%), and the double-row suture bridge technique were performed in 113 shoulders (83.7%). All the patients’ JOA and UCLA scores improved significantly from 69.0±11.8 and 15.9±5.0 points preoperatively to 88.0±11.2 and 29.0±5.9 points at 1 year postoperatively (p=0.049 and p=0.006, respectively). In this study, postoperative retears were noted in 15 of the 135 shoulders (11.1%) at 1 year postoperatively (Table 1).
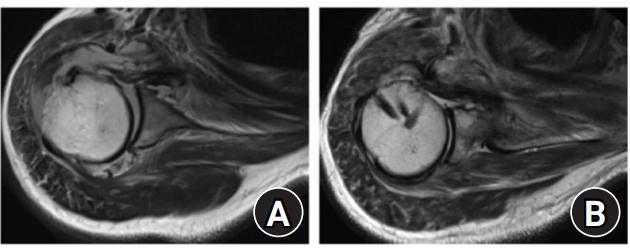
PD was observed in 10 patients (7.4%) preoperatively (Fig. 1) but not (0%) postoperatively. Among these 10 patients with preoperative PD, seven retears were observed. We noted a significant correlation between PD and retear (p<0.001; odds ratio, 34.1; 95% confidence interval [CI], 7.4–157.7). In all preoperative PD patients, the postoperative MRI scans showed PD improvement and HH centralization (Fig. 3). Regarding PD analysis reproducibility, Cohen’s κ values were 1.0 and 0.92 (95% CI, 1.0–1.0 and 0.81–1.0, respectively) for intra-observer and inter-observer agreement, respectively.
According to the DeOrio and Cofield classification, small/medium and large/massive tears (<3.0 cm and ≥3.0 cm, respectively) were observed in 98 and 37 shoulders, respectively (72.6% and 27.4%, respectively). The retear rate in the patients who had large/massive tears (12 retears/37 shoulders, 32.4%) was significantly higher than that in those who had small/medium tears (three retears/98 shoulders, 3.1%; p<0.001; odds ratio, 15.2; 95% CI, 4.0–58.0). The preoperative PD rate in the large/massive tear group (8 PD/37 shoulders, 21.6%) was significantly higher than that in the small/medium tear group (2 PD/98 shoulders, 2.04%) (p=0.001).
According to tear morphology, 53 anterosuperior tears (39.3%) and 43 posterosuperior tears were observed in this study. There was no significant correlation between preoperative PD and tear morphology (p=0.34). According to intraoperative findings, the LHB was intact in 28 shoulders (20.7%), injured in 92 shoulders (68.1%), and absent in 15 shoulders (4.3%). Surgical procedures were performed as below: preservation of LHB (n=41, 30.4%), LHB tenotomy (n=82, 60.7%), and LHB tenodesis (n=12, 8.9%). No significant correlation was observed between PD and LHB morphology/surgical procedures. (p=0.74 and p=0.42, respectively). No significant correlation was also detected between PD and the Hamada classification (p=0.23). Eight PD (6.5%) were observed in Hamada grade 1 (n=124), two PD (20%) in grade 2 (n=10), and none in grade 3 (n=1).
Low-grade Goutallier stages (stages 0–2) were seen in the SSCs, SSps, and ISps of 129, 118, and 133 shoulders, respectively (95.6%, 87.4%, and 98.5%). Preoperatively, high-grade Goutallier stages (stages 3 and 4) were seen in the SSCs, SSps, and ISps of 6, 17, and 2 shoulders, respectively, (4.4%, 12.6%, and 1.5%). The retear rate in the patients who had a high-grade Goutallier stage in any of the rotator cuffs (8 retears/23 shoulders, 34.8%) was significantly higher than that in those who did not (7 retears/112 shoulders, 6.3%; p<0.001; odds ratio, 8.0; 95% CI, 2.5–25.3). Significant correlations were observed between PD and the Goutallier classification of SSp and ISp but not with that of SSC (p=0.002, p<0.001, and p=0.311, respectively).
DISCUSSION
This study showed that 7.4% of RCT patients had PD preoperatively; as a result, PD could be recognized as a common MRI finding of RCT. PD had significant correlations with tear size and FD of SSp/ISp. Hence, it is understandable that these patients with PD had significantly higher postoperative retear rate in this study (70%; odds ratio, 34.1). The severity of RCT could be a reason for PD occurrence, and this could be a reason why PD is not found in all RCT patients. Although LHB is considered as a stabilizer of the shoulder joint, this study did not detect a significant correlation between arthroscopic LHB findings and preoperative PD. Particularly, ISp contributes to posterior stability of shoulder joints, and loss of this contribution could lead HH posterior shift in the supine position.
There are no specific methods needed to recognize PD; it can easily be seen on the axial view of a regular MRI scan in a clinical setting, and PD analysis reproducibility was excellent in this study. Therefore, we consider PD as a predictor of retear after ARCR, as well as tear size and FD of the torn rotator cuffs [13,18,19].
Typically, HH decentralization appears as antero-superior migration in patients with rotator cuff dysfunction [2,3]. The Hamada classification describes the progression of cuff tear arthropathy as a gradual decrease in acromiohumeral interval. In this study, no significant relationship between PD and the Hamada classification was detected. Contrastingly, the Walch classification describes posterior HH subluxation and posterior glenoid fossa wear as the result of HH decentralization in degenerative disease [20,21]. In patients with rotator cuff dysfunction, PD can occur as a pre-stage pathology as a result of a similar mechanism to that of posterior HH subluxation in degenerative disease. Although posterior HH subluxation in degenerative disease is currently described as a percentage change from the midline of the scapula [22,23], PD in RCTs is a subtle change. Therefore, we defined PD as a greater than 2 mm posterior shift of the HH to the scapula, based on past studies [8,9].
Interestingly, all the patients with preoperative PD improved postoperatively. Thus, we recognized that PD has no direct influence on postoperative retear after ARCR. Here, as both PD and retear were significantly correlated with preoperative tear size (≥3.0 cm) and with high-grade FD (Goutallier classifications 3 and 4), we propose that a spurious correlation exists between PD and retears after ARCR. Considering the high retear rate, PD can present a difficult situation to arthroscopic rotator cuff treatment. Other procedures such as tendon transfer, superior capsular reconstruction, or reverse shoulder arthroplasty are alternative treatment options for RCT with PD [24,25].
Our study had some limitations. First, because of the small number of patients with PD, it lacked adequate statistical power required to evaluate the outcomes. Second, the nature of this retrospective cohort resulted in inherent biases related to follow-up and measurement. Third, we did not evaluate the correlation between superior migration amount and PD. Resolution of these issues will provide further clarification as to the outcomes obtained.
PD is a common MRI finding in patients with RCT and is significantly correlated with tear size, FD, and postoperative retears after ARCR. PD might be a predictor of retear after ARCR. Moreover, PD can complicate arthroscopic repair, and an appropriate treatment for PD should be established.