INTRODUCTION
Scapular spine fracture is a serious complication of reverse total shoulder arthroplasty (RTSA) and often is caused by trauma or of insidious onset with no explicit trauma. The incidence of scapular fractures occurring after RTSA was reported to be between 1.3% and 10.2% [1-4]. In a particular study, 400 RTSA patients were analyzed and three discrete scapular fracture patterns were described: avulsion fractures of the anterior acromion (type I), fractures of the acromion posterior to the acromioclavicular joint (type II), and fractures of the scapular spine (type III) [1].
The mean time from diagnosis to surgery can be up to 9 months (range, 1.3ŌĆō24 months). Regardless of treatment, both conservative and surgery patients reported inferior function after fracture compared with initially after RSA [2,4-6]. Osteoporosis increases the risk of fracture [7]. Although it has been attempted to link surgical technique (baseplate orientation, screw length, and distance from screw tip to edge of bone) or other parameters (e.g., intact rotator cuff or design changes like lateralized humeral stem or glenoid side leading to an increase in deltoid stress) to the etiopathogenesis of postoperative acromion or spine fracture, no such associations have reached statistical significance. However, 41%ŌĆō57.1% of the fractures occurred in association with the tip of the long superior or posterior screw [2,5,7]. A recent biomechanical study reported a lower failure load with superior plus inferior metaglene screw constructs compared to the only inferior screw group, with a failure mode of scapular fracture rather than spine or acromion fractures seen clinically [8].
There is no study in the literature concerning the effect of baseplate superior or posterior screw fixation of the scapular spine on the occurrence of type 3 (base of scapular spine) fractures. The purpose of the present study was to compare the effects of long superior and/or posterior screws protruding and penetrating into the scapular spine on the strength of the scapular spine in a fresh cadaveric scapular model. The hypothesis was that a long outside-in superior baseplate screw will lead to scapular base fracture, and further long posterior outside-in screw fixation will cause fracture at lower load compared to a shorter screw.
METHODS
This study was approved by the Institutional Review Board of Dokuz Eyl├╝l University.
Fourteen fresh frozen cadaver shoulders cadaver shoulders shoulders were used for this study. The mean age of the cadavers was 68┬▒8 years (six female and eight male). There were no signs of fracture or macroscopic damage to any tendons or joint surface. The cadavers were allowed to thaw at room temperature overnight before testing and dissection.
Seven scapulae were allocated to the control group (short posterior and superior screw), while seven scapula were in the study group (four long superior screw+long anterior screw [L1], three long superior+long posterior screw [L2]). All long superior and long posterior screws were inserted to the scapular base, and all long anterior screws were inserted to the coracoid base. At least two long screws were planned to be used in the long screw group. One of these long screws was the superior screw to be inserted from the inside-out and targeting the scapular spine. Further, the other long screw was inserted from the anterior by targeting the coracoid basis through the bone (L1) or from the inside to the outside posteriorly, again targeting the scapula spine (L2). In the L1 group, the focus was to minimize the effect of the screw on spine breakage by sending it to the second long coracoid head from the anterior. All surgeries were performed by the lead author. The same 38-mm glenosphere baseplate (DePuy Synthes, Raynham, MA, USA) was used. The metaglene should ideally be positioned on the lower circular area of the glenoid bone. The metaglene central peg is positioned in the center of the inferior circle of the glenoid. The vertical metaglene marking was aligned with the base of the coracoid process superiorly. A 42 mm├Ś3.5 mm screw was used as the long screw, and the short screw was 22 mm├Ś3.5 mm. X-ray and gross inspection were performed to verify screw location.
The scapulae were cemented into a wooden block after being positioned with a frame. The scapulae were mounted to a materials testing system (AG-I 10 kN; Shimadzu, Kyoto, Japan) with the aid of a customized bone-cement junction conus covering the acromion but without contact with any part of the spine. This approach was used to achieve greater physiological force transmission along the length of the acromion compared to single-point loading (Fig. 1) [9]. A 1-N preload was applied for 10 seconds, and each specimen was loaded at a constant rate of 0.5 mm/s until fracture of the acromion or base of the spine. The load (N) versus displacement (mm) was recorded until failure. The ultimate tensile load was considered the peak force. Stiffness was calculated by determining the slope of the loadŌĆōdisplacement curve with the use of a best-fit line on the load versus displacement curve. The ultimate load (N) and stiffness (N/mm) were measured.
Statistical Analysis
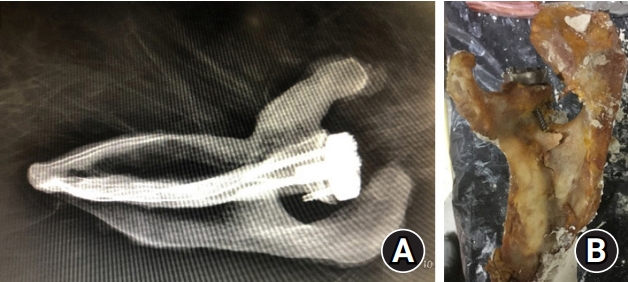
Data analysis was performed using IBM SPSS ver. 20.0 (IBM SPSS Corp., Armonk, IL, USA). The Mann-Whitney U-test was used to analyze the difference between the mean values of tested variables among the groups. First, the spine fixation group (n=7) was compared with the control group (n=7). Then the spine fixation group with a base of spine (type 3, n=6) fracture (Fig. 2) was compared with the control group. A post-hoc power analysis was performed for the spine fracture group in comparison with the control group. A p-value less than 0.05 was considered statistically significant.
RESULTS
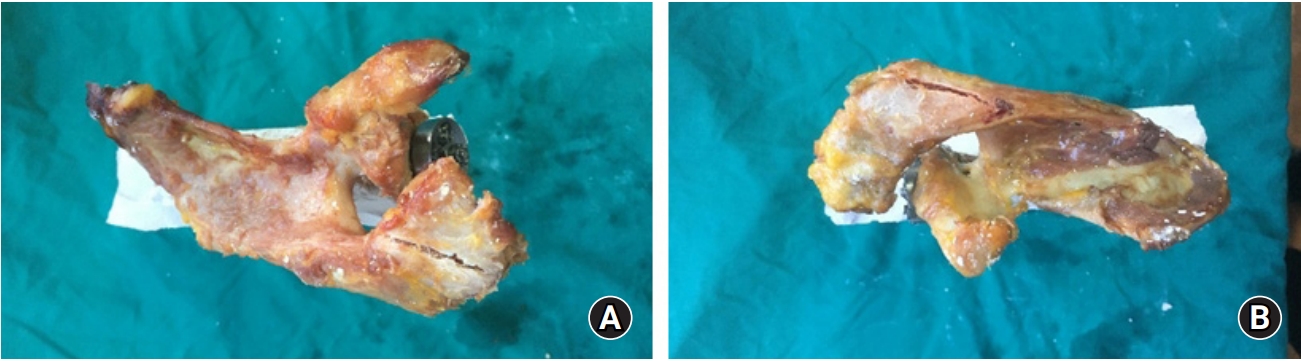
Specimen data are given in Table 1. All specimens in the long screw group except specimen number 7 (long superior and long anterior screws) in the L1 group failed due to acromion spine fracture (type 3) (Fig. 3). In the short screw group, specimen number 7 failed due to acromion fracture (types 1 and 2) (Fig. 4 ). There was no significant difference in mean ultimate load and stiffness when the long screw group was compared to the short screw group (p=0.27, p=0.8). This was similar when specimen number 7 at L1 was excluded (no outside-in screw, failure type 1; n=6) and compared to the short screw group (p=0.25, p=0.77, respectively).
The mean load and stiffness tended to be lower for L1 compared to L2. Specimen number 13 in the L2 group had superior screw performance without an outside-in configuration (all inside at the base of spine), while a posterior screw having outside-in fixation into the scapular spine failed with scapular spine base fracture (type 3). A post-hoc power analysis for spine fracture (n=6) comparison to the short screw group (n=7) yielded 0.18 (%) for ultimate load and 0.064 (%) for stiffness.
DISCUSSION
The main finding of the study was that when the superior metaglene screw (with or without a posterior or anterior screw) enters into the base of the spine with an outside-in configuration, it leads to a fracture at the base of the scapular spine compared to the short screw ŌĆ£not touching the scapula spineŌĆØ group, which failed due to acromion fracture. Only one specimen (No. 7 in the L1 group) did not cause a scapula spine base fracture due to fixation of the spine base without an outside-in configuration. However, due to the small number of specimens, the present study failed to show a decrease in ultimate load of the acromion spine when two long screws were used instead of two short screws.
Many clinical studies have highlighted the possible relationship between long superior or posterior screws and later occurrence of scapula spine base fracture [2,5,7]. However, due to the small number of occurrences, statistically significant conclusions could not be made [2,5,7]. A recent review also pointed out how scapula spine stress fracture might be related to malposition of the superior 12 oŌĆÖclock and the posterior (9 oŌĆÖclock) screws [1]. They advocate that the superior screw be Ōēż24 mm and angled into the base of the coracoid to prevent nerve injury due to extraosseous placement [10-12]. This was also true for the posterior screw. They advocate avoiding long posterior screws (Ōēż20 mm) to prevent breaching of the spinoglenoid notch and injuring the suprascapular artery and nerve with possible scapular spine fracture.
Whatever treatment is chosen, inferior function is reported after fracture compared with immediately after RSA [2,5,6]. Type 3 fracture (base of acromion spine) especially is associated with painful non-union, which might lead to a greater need for surgical intervention [1]. A recent biomechanical study favored locking the compression plate instead of the lateral clavicular plate or reconstruction plate [9].
There is only one biomechanical study in the literature describing the relationship between superior screws and scapula fractures. Kennon et al. [8] reported that one additional superior screw in addition to the inferior screws led to lower scapula failure load (1,077 N vs. 1,970 N), similar to that in our short screw group. They used embalmed cadaveric specimens instead of fresh, as were used in the present study. Their test apparatus was direct compression force from the humerus to scapula. The resultant failure mode was scapula fracture instead of acromion or scapula spine-based fracture, which is the type seen clinically, differing from the present study. The metaglene used in that study was unique in that it had six holes allowing three screws to be placed below the central cage. However, most implants on the market use four screws, one to be placed below the central cage [8].
Some limitations exist for this study; for example, the force applied on the superolateral aspect of the acromion does not fully reflect the distribution of forces acting on the acromion during active shoulder mobilization after RTSA. Further, the majority of scapula and acromion fractures after reverse arthroplasty is stress-related and atraumatic. However, we fractured the acromion or base of spine and correlated the base fracture to the long outside-in screw testing. Additionally, the testing protocol used in the present study was verified in a previous study, and it mimics physiological deltoid muscle pull on the acromion [9].
Second, this is a biomechanical study aimed to test the strength of a construct at time zero and not the healing response over time. Although there was no macroscopic evidence of damage to any component of the joint, there is a possibility that bone quality differences exist between the specimens tested. Additional bone mineral testing would add useful information regarding interpretation of the results. The supply of fresh frozen human cadavers is limited, and the number of specimens in each group was low (n=7). This low sampling rate prevents conclusion with certainty that the long posterior screws decrease the strength of spine and/or lead to fracture at lower loads. However, other biomechanical studies have utilized six specimens per group [13-16]. Specimen number 13 in the L2 (superior screw ŌĆ£all inside,ŌĆØ posterior screw outside-in) group failed at higher load than specimen numbers 10 and 12, which had both screws with outside-in fixation into the scapular spine. Third, samples could not be prepared using the two shoulders of one cadaver because the fresh frozen cadavers were separated only in the form of the upper extremities. Furthermore, the bone quality of cadavers was not measured, so the groups were randomly assigned.
The present study indicates the need for additional studies. First, does this outside-in configuration cause spine base fracture using a more physiological test set-up or in a clinical scenario? Second, can all-inside superior long screws aiming toward the scapular spine base be applied clinically and/or prevent fracture of the scapular spine while increasing fixation strength of the baseplate? Third, does an additional outside-in posterior screw further decrease spine fracture load?
Outside-in long superior screw fixation of the base of the scapular spine led to a base fracture compared to the short screw group, which failed due to acromion fracture. The present study points out the significance of prevention of cortical breach or outside-in configuration when the scapular spine base is fixed with superior or posterior screws.