INTRODUCTION
Distal humerus fractures (DHFs) account for approximately 30% of all elbow fractures [1,2] with an incidence of 5.7/100,000 per year [1]. Treatment can be challenging due to the complex anatomic structure of the elbow joint and surrounding nerves, tendons and ligaments. Most DHFs are treated with open reduction and internal fixation using a double plating technique. Exposure of the articular surface of the elbow joint is important for successful anatomical reconstruction. However, due to the complex ligamentous anatomy and proximity of neurovascular structures, achieving adequate surgical exposure can be challenging.
Multiple approaches such as the triceps-splitting approach [3] and the triceps-sparing approach [4] have been described. Even though âtriceps-onâ approaches are gaining popularity, the most commonly used approach is to expose the distal humerus by performing olecranon osteotomy. Osteotomy increases exposure of the articular surface by 11%â22% compared to a triceps-splitting or -reflecting approach [5]. The osteotomy site is later fixed using tension band wiring, a screw, or a plate. Complications of olecranon osteotomy are commonly reported, including failure or pull out of the hardware used for fixation, which can result in malunion or non-union, skin penetration, infection or stiffness [2,6]. Although olecranon osteotomy is widely used by upper extremity and trauma surgeons, little is known about the frequency of associated complications. Better insight into the type and frequency of complications can aid surgeons in thoroughly informing their patients of the risks of this type of surgery. The aim of this study was to clarify the type and frequency of complications that occur after olecranon osteotomy in the treatment of DHFs and to evaluate the relative effectiveness of different types of osteotomy fixation.
METHODS
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [6]. This review was registered in the PROSPERO (International Prospective Register of Systematic Reviews; registration number: RD42020150115).
Search Strategy and Criteria
A literature search was conducted in the PubMed/Medline, Embase, and Cochrane Library digital databases up to February 2020 to find articles that described complications or repeat operations among patients with DHF treated using the olecranon osteotomy approach. Search terms that were used were: ((((âOlecranon Processâ[Mesh] OR olecranon*[tiab])) AND ((âHumerusâ[Mesh] OR humerus[tiab] OR humeral[tiab]) AND (âFractures, Boneâ[Mesh] OR fractur*[tiab])))) NOT (((âOlecranon Processâ[Mesh] OR olecranon*[tiab])) AND (âOsteotomyâ[Mesh] OR osteotom*[tiab])).
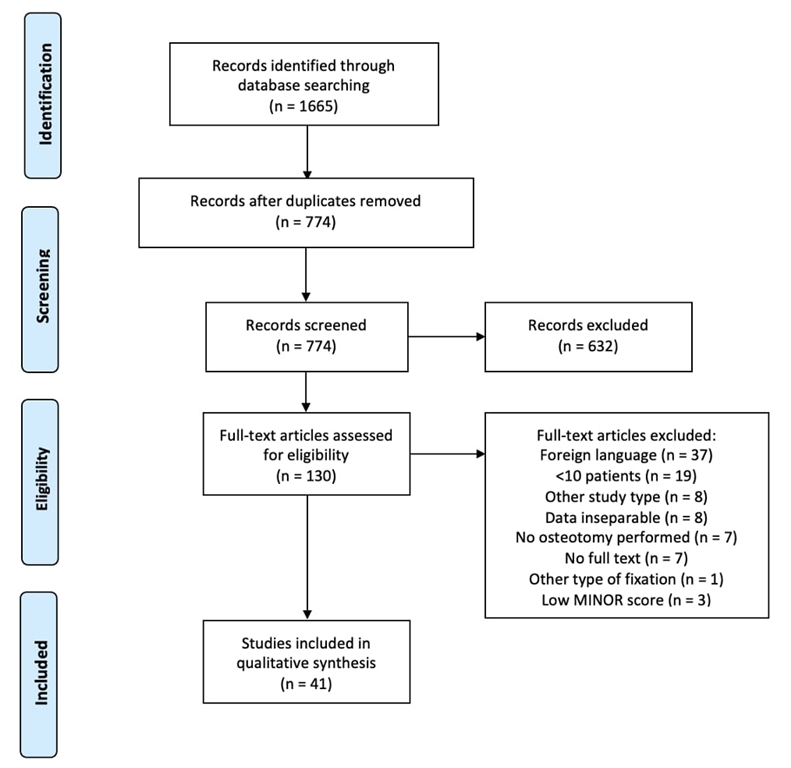
Two reviewers (KES and BJS) independently reviewed the articles by title and abstract screening. Duplicates were removed and titles were initially screened. One hundred thirty-one articles remained for whole-text screening; 90 of these were excluded, leaving 41 papers for in-depth evaluation (Fig. 1).
Inclusion and Exclusion
Studies were included in the systematic review if more than 10 patients with olecranon osteotomy in the surgical treatment of a DHF were included, patients were over 18 years old, and complications were described. Exclusion criteria were: (1) case reports, review articles, letters to the editor, conference abstracts, instructional courses, and animal/cadaver/in vitro studies; (2) a pediatric population; (3) lack of separate data on complications of olecranon osteotomy; (4) olecranon osteotomy used for treatment of other elbow pathology; (5) incomplete text; or (6) methodological index for non-randomized studies (MINOR) score lower than 10.
Assessment of Study Quality
The methodological quality of the included articles was tested by two separate reviewers using the MINORS criteria [7] in which comparative and non-comparative studies are assessed for quality through a point system in which items that are required to be described are scored. The global ideal score is 16 for non-comparative studies and 24 for comparative studies.
Data Extraction
Two reviewers (KS, BS) independently extracted data from each study using a predefined data extraction form. Two primary researchers (KS, BS) examined each of the articles independently and the senior author (MPJ van den Bekerom) resolved any disagreement. We extracted patient characteristics (sex and age, fracture classification, open or closed fracture, type of surgery, and type of fixation), study specific data (date of publishing, type of study, number of patients included, enrollment period, and duration of follow-up) and complication rate and type (wound complications, hardware failure, malunion or non-union, and removal of hardware).
Statistical Analysis
Data were analyzed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA). The Kruskal-Wallis test was used for testing differences in complication rates between different fixation techniques of the osteotomy site. Data are shown as percentages and means with ranges and standard deviations.
RESULTS
A total of 1,665 articles were found using the described search criteria. After the duplicates were removed, 774 articles remained for screening. Another 632 articles were excluded, after which 131 full-text articles were assessed for eligibility. After full-text screening, 86 articles were excluded. Three more articles were excluded based on their low MINOR score, and one was excluded because of a different fixation technique of the osteotomy site. A total of 41 articles [8-48], including six prospective studies, were included in the qualitative synthesis. Articles were published between 1994 and 2020 and included 10 or more (upper limit of range, 184) osteotomies. Further information can be found in the flow diagram. Mean MINORS score was 13.4 (10â20). In these 41 articles, a total of 1,700 osteotomies in 2,030 patients were described. There were 997 males (48.8%), and the mean age was 45.3 years (range, 12â97 years). Fracture characteristics can be found in Table 1.
The mean time between injury and surgery was 1.7 days and the mean follow-up time was 22.6 months (range, 3â156 months). Most osteotomies were fixated with tension band wires (n=660), others were fixed with wires and screws (n=320), plates (n=114), and screws (n=6). Gofton et al. [22] described one case in which the osteotomy site was not fixated.
A total of 447 complications were reported. Of these 447 complications, 71 (4.2%) were wound infections, ranging from 0% to 23%. Of these, 23 (1.4%) were deep infections and 48 (2.8%) were superficial. Delayed union occurred in 29 osteotomies (1.7%), specified up to 14 months. There were 34 (2%) non-unions, and one (0.1%) malunion of the osteotomy site was described by Mardanpour and Rahbar [33]. Non-union was only specified by Schmidt-Horlohe et al. [39] (radiolucency at more than six months follow-up in association with pain) and Woods et al. [47] (radiolucency at more than nine months of follow-up). Other incidental complications, such as ulnar neuropathy, hardware failure, heterotopic ossifications and removal of hardware are described in Table 2. The only significant difference was in ulnar nerve neuropathy, which was found more frequently in osteotomy fixed with screws.
DISCUSSION
Olecranon osteotomy is a widely used approach in the surgical treatment of DHFs to establish adequate exposure of the articular surface of the distal humerus. However, this approach has high complication rates. As an alternative, less invasive techniques with potentially lower complications rates, such as the paratricipital approach, can be used [10,20,40,48]. To provide surgeons with better information on the incidence of complications related to this approach, we aimed to synthesize studies on this common approach. Therefore, this paper provides a systematic overview of the complication rate related to olecranon osteotomy in the surgical treatment of DHFs. Our data revealed that the olecranon osteotomy approach is not as forgiving as currently taught to orthopedic surgeons in training: the complication rate related to an olecranon osteotomy in the setting of DHF is high. Serious problems, such as wound infections (3.3%), delayed or non-union of the olecranon osteotomy (3.6%), ulnar neuropathy (5.5%), hardware failure (1.1%) and heterotopic ossifications (1%) are frequently encountered.
Use of olecranon osteotomy may not always be appropriate. However, in comminuted DHFs, the paratricipital approach does not provide sufficient exposure of the fracture and the joint; in these fractures, surgeons may prefer olecranon osteotomy for advanced exposure.
Difficulty achieving union can be related to inadequate reduction in complex DHFs that cannot be reconstructed anatomically, resulting in stress on the osteotomized olecranon. Delayed and non-union can also be the result of insufficient fixation. A next step in non-union of DHF can be a total elbow prosthesis. However, in the case of an earlier olecranon osteotomy, this is a more difficult surgery because of the cement that migrates into the osteotomy. In studies that compare the olecranon osteotomy approach to the triceps-splitting, triceps-lifting (paratricipital) or triceps-sparing approach, complications tend to be higher in the group that is treated via the olecranon osteotomy approach [10,20,40,48]. This may be due to the longer duration of surgery in addition to the implantation of material for osteosynthesis of the osteotomy site. Also, since the olecranon osteotomy is used more frequently in more serious fractures, these results may have been affected by bias. Based on our systematic review, 2.8% of patients had a superficial infection; however, a âsuperficial infectionâ was not well defined in most studies. As the olecranon is covered by a thin layer of skin, the osteotomy site is prone to rubbing of fixation materials, resulting in skin irritation. This can cause superficial or even deep infection. Because of the thin, soft tissue envelope of the olecranon, defining all infections as deep infections may be a safer approach.
To the best of our knowledge, this is the first review focused on complications related to olecranon osteotomy in the surgical treatment of DHF. Olecranon osteotomy is not as safe as generally considered; its high complication rate should not be underestimated. Articles comparing olecranon osteotomy to paratricipital tend to report higher complication rates, ranging from 45.8% to 55% in patients treated via the olecranon osteotomy versus 27.2% to 40.6% in patients treated via the paratricipital approach [11,20,40]. Complications related to osteotomy, such as delayed or non-union, hardware failure, and symptomatic removal of hardware, are prevented when the paratricipital approach is used. These preventable complications may require additional surgical interventions. This may discourage the use of olecranon osteotomy because the functional outcome of the paratricipital approach is often comparable to that of olecranon osteotomy. The complication rate might be underestimated, as detailed analysis with three-dimensional computed tomography is not available in most studies. As an osteotomy of the olecranon compromises the articular anatomy in most procedures, small articular steps and gaps and subtle malunion are not detected on simple radiographs, but may still cause posttraumatic osteoarthritis.
A limitation of this study is that some articles failed to separate data based on respective fixation type. Furthermore, not all articles described fracture characteristics and all types of complications. These data were not included in statistical analysis for the differences in complication rate. In this study, four different types of fixations were described: tension band wiring, screws with or without tension band, and plate fixation. No statistically significant differences were found in complication rates between these different fixation types except that more frequent ulnar nerve neuropathy was observed in osteotomies fixated with screws. However, since this was not specifically assessed in all articles, we cannot classify this as significant. Ulnar nerve neuropathy may be caused by the fixation of the osteotomy or the fixation of the fracture. We have concluded that there is no superior method for fixation in olecranon osteotomy. Randomized controlled trials (RCTs) testing the effectiveness of tension band wiring versus plate fixation are not yet available. Both tension band wiring and plate fixation of the osteotomy site have technical failures such as pull out or migration. Patients must be monitored frequently for wound healing and to identify and treat complications at an early stage. More high-quality research, such as a multi-center RCTs or a national database describing DHF treatment and outcomes, is needed to clarify the advantages and disadvantages of each technique.
Olecranon osteotomy is a frequently used approach that provides extended exposure of the articular surface of the distal humerus. However, the high risk of complications related to this approach must be considered in the decision to perform an osteotomy and/or to opt for âtriceps-onâ approaches. The advantages of the limited exposure increase do not outweigh the drawbacks and complications associated with this technique. Awareness of alternatives, such as the paratricipital approach, which has fewer complications and comparable functional outcomes, is essential. When selecting olecranon osteotomy, patients must be well-informed pre-operatively and monitored closely postoperatively to assess and treat possible complications at an early stage.