Introduction
Open reduction and internal fixation (ORIF) to restore the articular surface is the conventional treatment for distal humerus fractures [1-3]. However, it is sometimes impossible to restore articular congruency (for example, in cases with osteoporotic bones or severely comminuted fractures), making the conventional option more challenging and less effective. Since complications and reduction loss rates as high as 50% have been reported after conventional ORIF for comminuted fractures [4], arthroplasty has been advocated as a suitable alternative in such cases. Elbow arthroplasty has been practiced since 20 years, with continuous improvements in technique and device design [5]. An increasing number of studies have reported results related to geriatric distal humerus traumatology, and total elbow arthroplasty (TEA) is now considered an important treatment option [4,6,7]. While TEA offers an alternative option to treat comminuted distal humerus fractures, complications (including aseptic loosening, periprosthetic fracture, and infection) continue to limit the utility of this procedure in younger patients. Distal humerus hemiarthroplasty may therefore be more suitable for younger patients since it offers a shorter surgical time, does not generate polyethylene waste, and has a lower risk of component loosening as compared to TEA.
Mellen and Phalen [8] first suggested the concept of hemiarthroplasty and made customized acrylic implants for young active soldiers with complex intra-articular fractures of the distal humerus at a US Army Hospital. The practice of hemiarthroplasty for complex distal humerus fractures has evolved since then [9-11]. While TEA is well described and reported, few studies have reported the outcomes of hemiarthroplasty for distal humerus fracture. Hence, there are no consensus guidelines for TEA indications or any reports on the outcomes to help elucidate age-dependent risks and benefits to guide management decisions. We found only one comparative systematic review of TEA versus distal humerus hemiarthroplasty, but the outcomes based on age and implant choice were not considered [12]. Thus, we aimed to analyze the clinical outcomes and complications associated with hemiarthroplasty using the single-implant system (the Latitude system) in distal humerus fractures through a systematic review of relevant literatures.
Methods
Search Strategy
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) checklist and algorithm [13] guided this systematic review of literature found in the databases of PubMed, Ovid MEDLINE, and Cochrane Library. We combined the terms ‘hemiarthroplasty’ OR ‘hemi prosthesis’ OR ‘hemi replacement’ OR ‘hemi’ OR ‘arthroplasty’ AND ‘distal humerus’ OR ‘distal humeral’ OR ‘distal humerus fracture’ OR ‘distal humeral fracture’ OR ‘elbow fracture’.
Inclusion/Exclusion Criteria
This review included studies of human subjects, with original data published in the English language that reported outcomes of hemiarthroplasty for distal humerus fractures, with a minimum follow-up of 1 year. Included studies were required to report clinical outcomes or complications after using the Latitude system for distal humerus fracture. Review articles and case reports were excluded.
Data Extraction
Data regarding study characteristics, patient demographics, indications and contraindications, inclusion and exclusion criteria, and outcome measures were extracted from each study that met the inclusion criteria. The literature search and data extraction were performed by 4 blinded reviewers. Articles published on or before June 15, 2017 were considered. Only papers published in peer-reviewed journals were eligible, and relevance was established on the basis of article titles and abstracts. After article selection, bibliographies were assessed by the reviewers to identify further relevant articles. Three reviewers (GBL, EK, and JMK) reviewed each paper independently and discussed and resolved any disagreements on the inclusion or exclusion of any articles. The inclusion and exclusion of studies were also discussed with an expert orthopedic surgeon (IHJ). Study characteristics of interest included author names, year of publication, study design, number of patients at the final follow-up, and length of follow-up. Patient demographics included sex and age. Outcomes of interest included postoperative functional outcome scores, radiographic assessment, complications, reoperations, and conversion to TEA. Descriptive statistics were used to report study characteristics, patient demographics, and outcomes.
Quality Assessment
The methodologic quality of the included studies was analyzed with the modified Coleman Methodology Score [14]. This score assesses the methodology of clinical studies using 10 specific quantitative and qualitative criteria: study size, mean follow-up, number of surgical procedures, type of study, diagnostic certainty, description of surgical procedure, postoperative rehabilitation, outcome measures, outcome assessment, and selection process. However, since this classification was originally designed for the knee, we partially modified the Coleman Methodology Score for appropriate assessment of the elbow. Potential scores range from 0 to 100, with a score of 100 indicating the highest study quality. The level of evidence of each study was determined using the Journal of Bone and Joint Surgery criteria.
Statistical Analysis
We also conducted a meta-analysis, for which the results using the random-effects model took into account the possible clinical diversity and methodological variations between studies. Specific analyses considering confounding factors were not possible due to unavailability of raw data. Categorical variables were expressed as frequencies with percentages, and continuous variables were expressed as mean values with ranges. Functional outcome and range of motion data were presented using standardized mean deviation calculations. All statistical analyses were performed with the IBM SPSS ver. 21.0 (IBM Co., Armonk, NY, USA). A pooling data analysis was performed using randomeffect models, which assumed that there were variations between studies. The chi-square tests studied the heterogeneity between trials. The I2 statistic was used to estimate the percentage of total variation across studies, owing to heterogeneity rather than chance, with values greater than 50% being considered as substantial heterogeneity. I2 was calculated using the following formula: I2=100%×(Q-df)/Q, where Q is defined as Cochrane’s heterogeneity statistic and df is defined as degree of freedom. The possible clinical and methodological reasons in cases of substantial heterogeneity were qualitatively explored.
Results
Our literature search and references scan identified 231 relevant articles; of these, 218 were excluded for various reasons as indicated (Fig. 1). Evaluation of the remaining articles excluded further 4 articles due to short follow-up durations (less than 1 year), other implants, and absence of full text. Ultimately, 9 articles were included in the final analysis.
Demographics
A total of 115 patients from the 9 articles were included in the study, most of whom were female (Table 1) [10,11,15-21]. Among the 9 included articles, 2 articles described 2 different implant systems (the Sorbie-Questor system and the Latitude system); based on the raw data of these articles, our analysis included only those cases where the Latitude system had been used.
Clinical Functional Scores
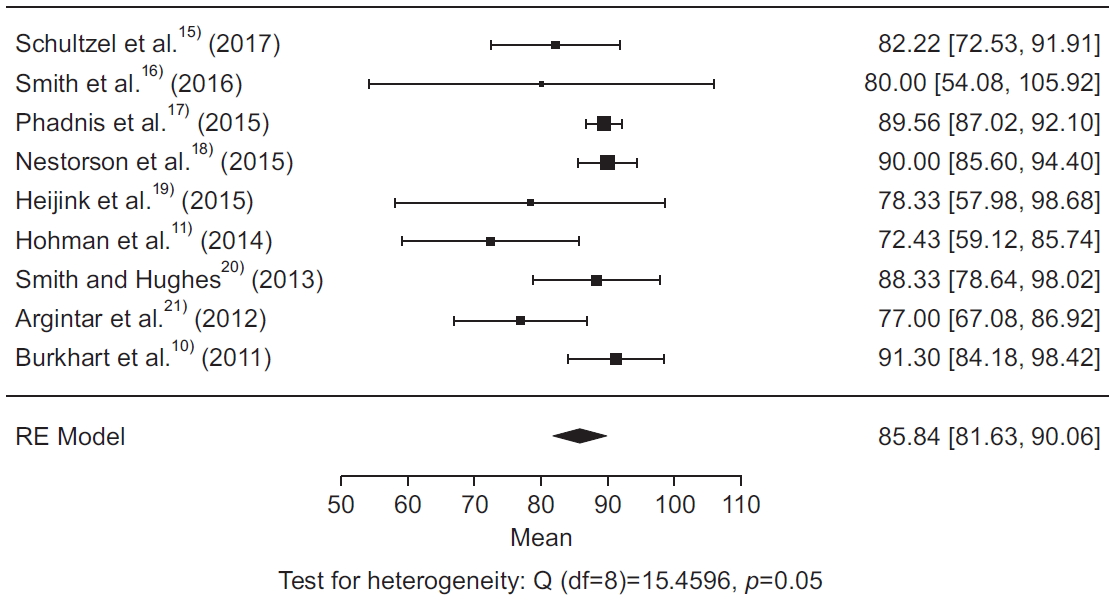
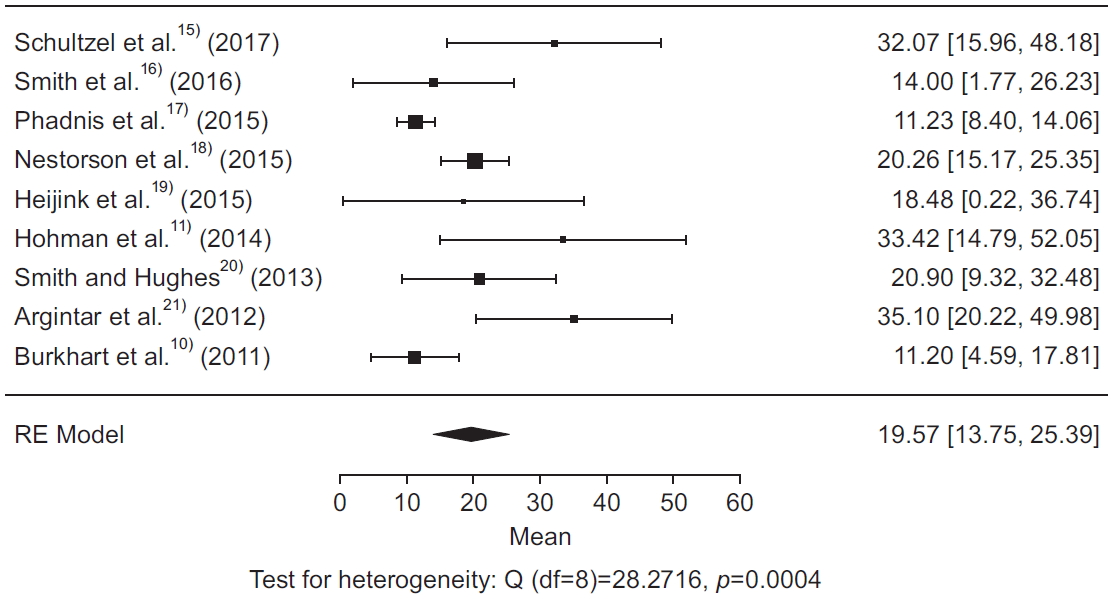
Most studies reported good or excellent outcomes, flexion-extension range of motion, and pronation-supination range of motion (Table 2). The weighted mean of Mayo elbow performance scores (MEPS) was 85.8 (I2=60.36%; heterogeneity), and the weighted mean Disabilities of the Arm, Shoulder and Hand (DASH) score was 19.6 (I2=74.76%; heterogeneity) (Fig. 2, 3).
Range of Motion
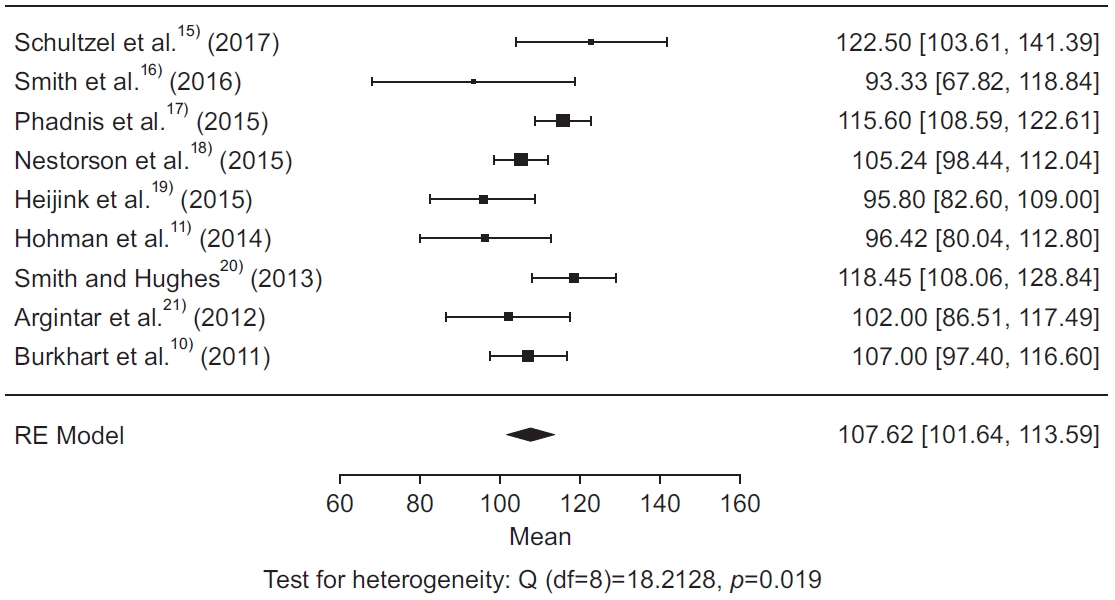
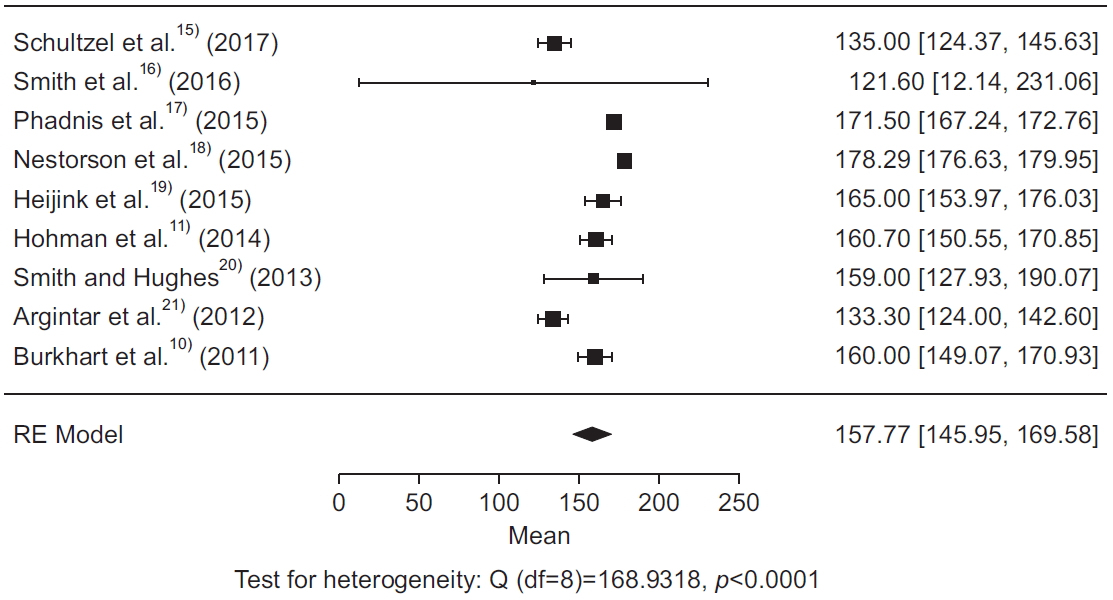
The weighted mean flexion-extension and pronation-supination arcs were 107.6° (I2=57.24%; heterogeneity) and 157.5° (I2=95.58%; heterogeneity), respectively (Fig. 4, 5). Considering that arc of motion 100° (30° of extension to 130° of flexion) and an arc of forearm rotation 100° (50° of pronation to 50° of supination) are required for activities of daily living, 76% of patients achieved a functional range of motion for flexion and extension, and 99% achieved functional pronation and supination (Table 2).
Complications
Overall, there were 85 complications among the 115 patients evaluated. Cartilage wear (n=45) was the most common complication reported, followed by heterotopic ossification (n=39), loosening (n=13), and neuropathy (n=11). Other lesser complications included fracture (either intra- or postoperative) (n=7), stiffness (n=6), posterolateral rotatory instability (n=4), continuous pain (n=2), peri-prosthetic infection (n=1) and wound breakdown (n=1) (Table 3).
Discussion
This systematic review focused solely on employing the Latitude system for hemiarthroplasty for distal humerus fracture. All the studies included are classified as level IV evidence. The generally accepted optimal treatment for distal humerus fractures is ORIF, which is able to achieve stable fixation in majority of fractures; however, once attempts at fixation have failed, conversion to hemiarthroplasty avoids suboptimal fixation leading to poor outcomes. Distal humerus hemiarthroplasty is most typically used for intra-articular fractures of the distal humerus in geriatric populations. It also serves as a salvage procedure in younger patients with rheumatoid arthritis or tumors. To the best of our knowledge, by investigating the data of 115 patients who underwent distal humerus hemiarthroplasty, our work represents the most complete analysis for this specific indication.
Our analysis revealed that patients undergoing distal humerus hemiarthroplasty were more likely female and mostly in their seventh decade of age (mean, 66.41 years). Functional outcomes were summarized by means of 85.84 and 19.57 for MEPS and DASH scores, respectively. These outcomes are comparable with results associated with TEA [22].
Distal humerus hemiarthroplasty offers several benefits when compared to TEA, including preservation of the bone stock as well as minimization of postoperative restriction or revision surgery. Distal humerus hemiarthroplasty also preserves the native collateral ligaments, which helps preserve elbow proprioception. As for any other hemiarthroplasty, cartilage wear remains the most common challenge.
Despite the advantages of distal humerus hemiarthroplasty, complication rates remain higher than TEA. The most common complication in our review was cartilage wear (39.1%), followed by heterotopic ossification (33%), loosening (11.3%), neuropathy (9.6%), and stiffness (5.2%). Others less reported complications were periprosthetic fracture (4.34%), instability (3.47%), wound necrosis (1.73%), hardware irritation (0.86%), and triceps muscle weakness (0.86%). A common concern with any hemiarthroplasty is wearing of the native joint at the articulation point, resulting from a disparity in elasticity and surface roughness between the articular cartilage and prosthesis lining. With altered loading, the cartilage wears with time, eventually manifesting as and later causing instability and inducing the toggling movements. Loosening is also a worrisome and frequent complication of arthroplasty. We postulate that the cementing technique specifically contributes to this complication. In this situation, the prosthesis pullout is perpetuated by the pistoning movement of the cement mantle. However, the loosening rate of hemiarthroplasty was lower than that observed in TEA [22].
The lack of standardized outcome measurements and consistent follow-up are limitations to our analysis. Published literature on distal humerus arthroplasty for distal humerus fracture is limited, and therefore our analysis lacks power. The case series that do exist are short, often with limited and irregular follow-up. We were unable to utilize certain statistical analysis methods, such as correlation testing, since the power of the test depends on the number of studies included. In a meta-analysis that includes less than 25 studies, the correlation test will be unable to withstand biases in the literature search.
This systematic review highlights the favorable outcomes of distal humerus arthroplasty for distal humerus fracture with the Latitude system. We propose that prospective analysis should be directed at forming regimented physical therapy to reduce complication rates.